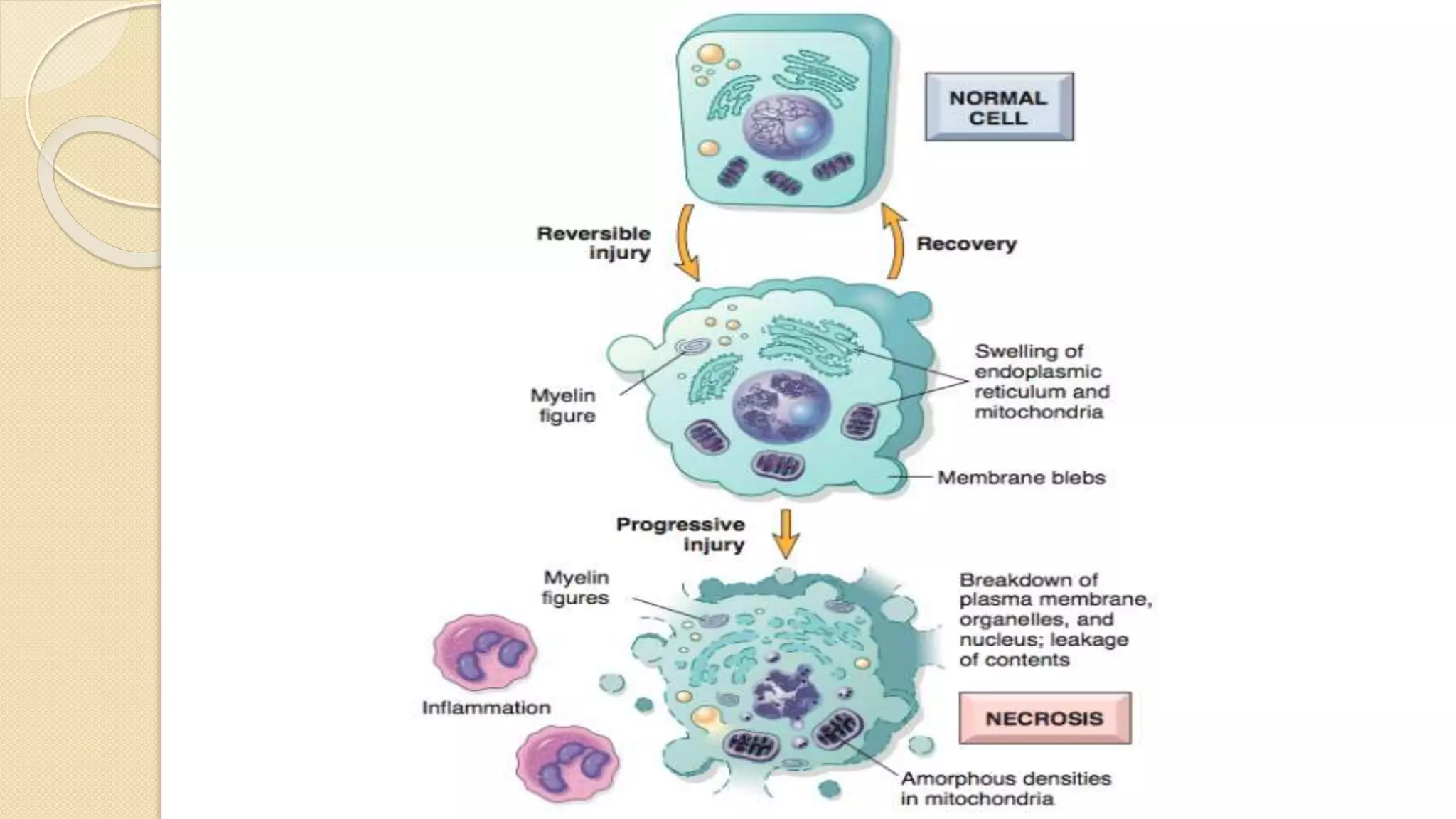
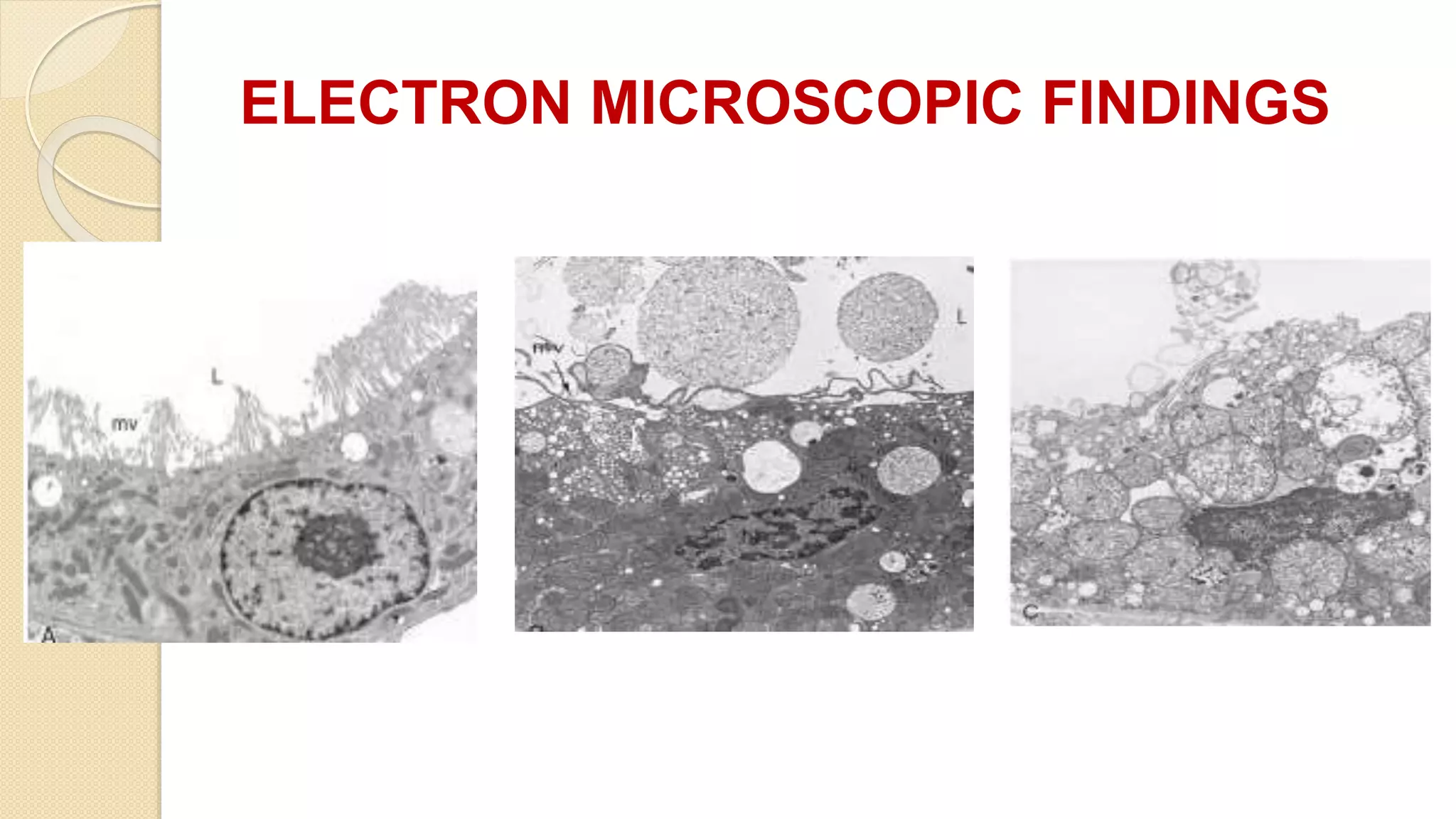
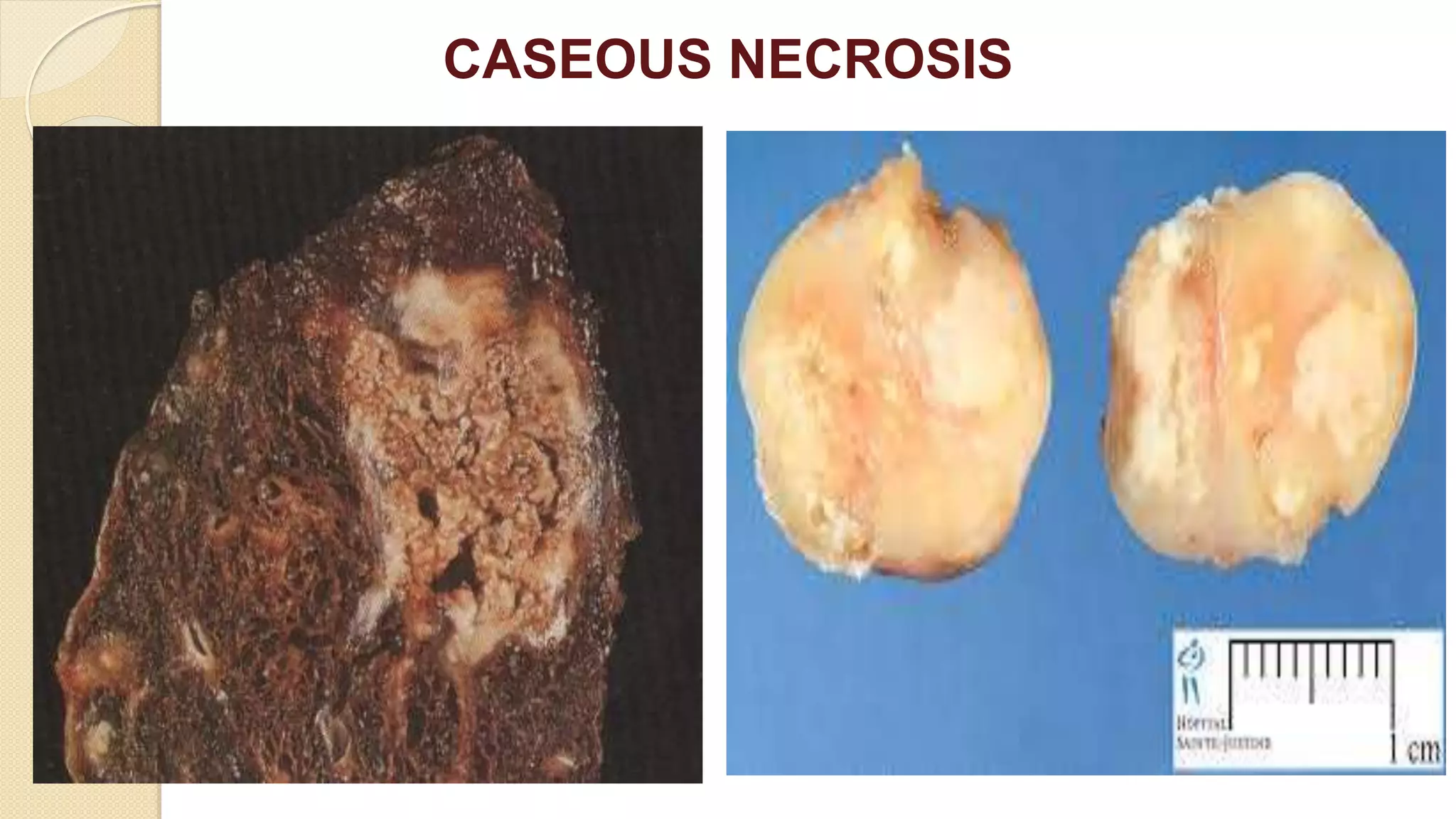
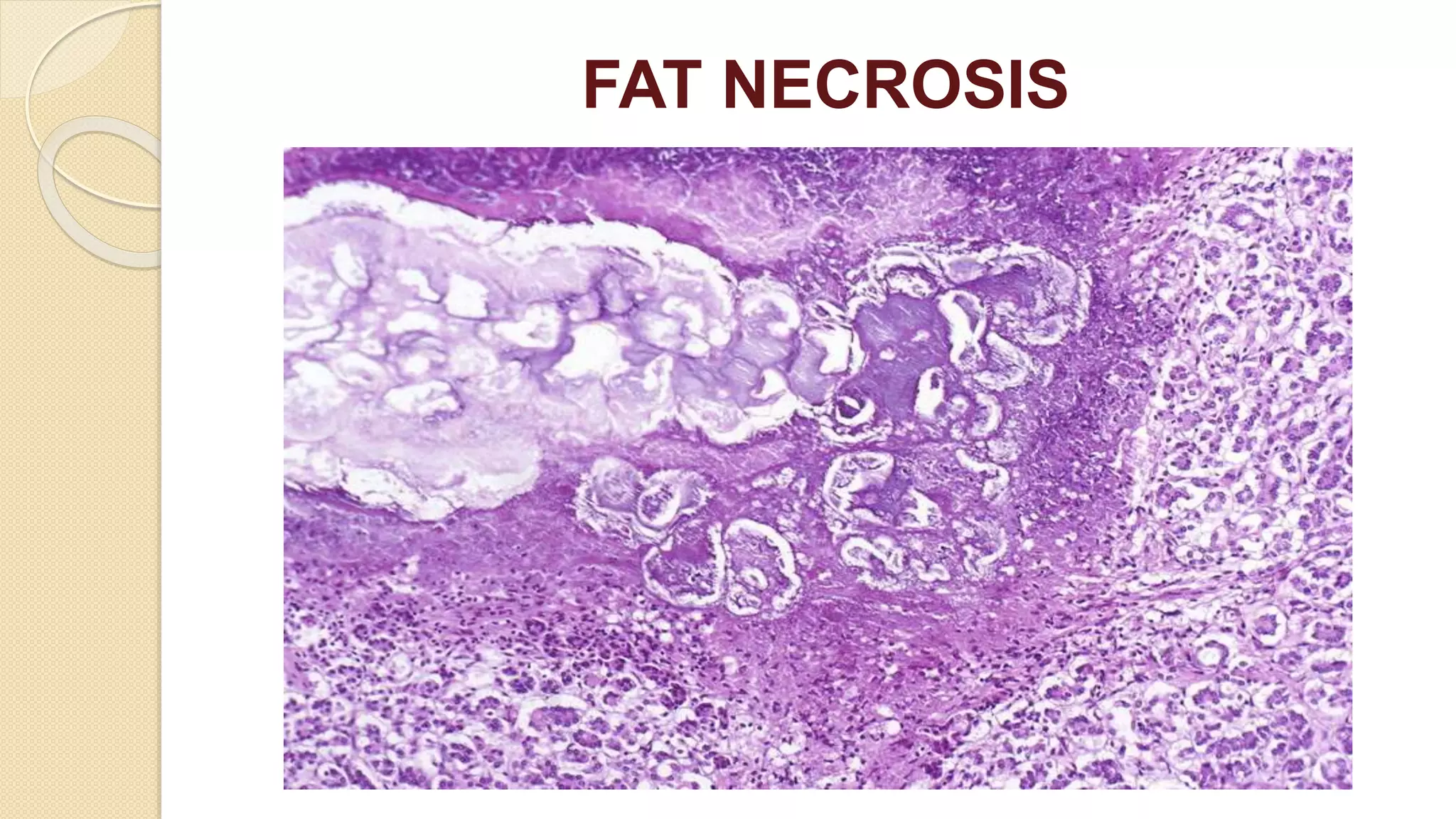
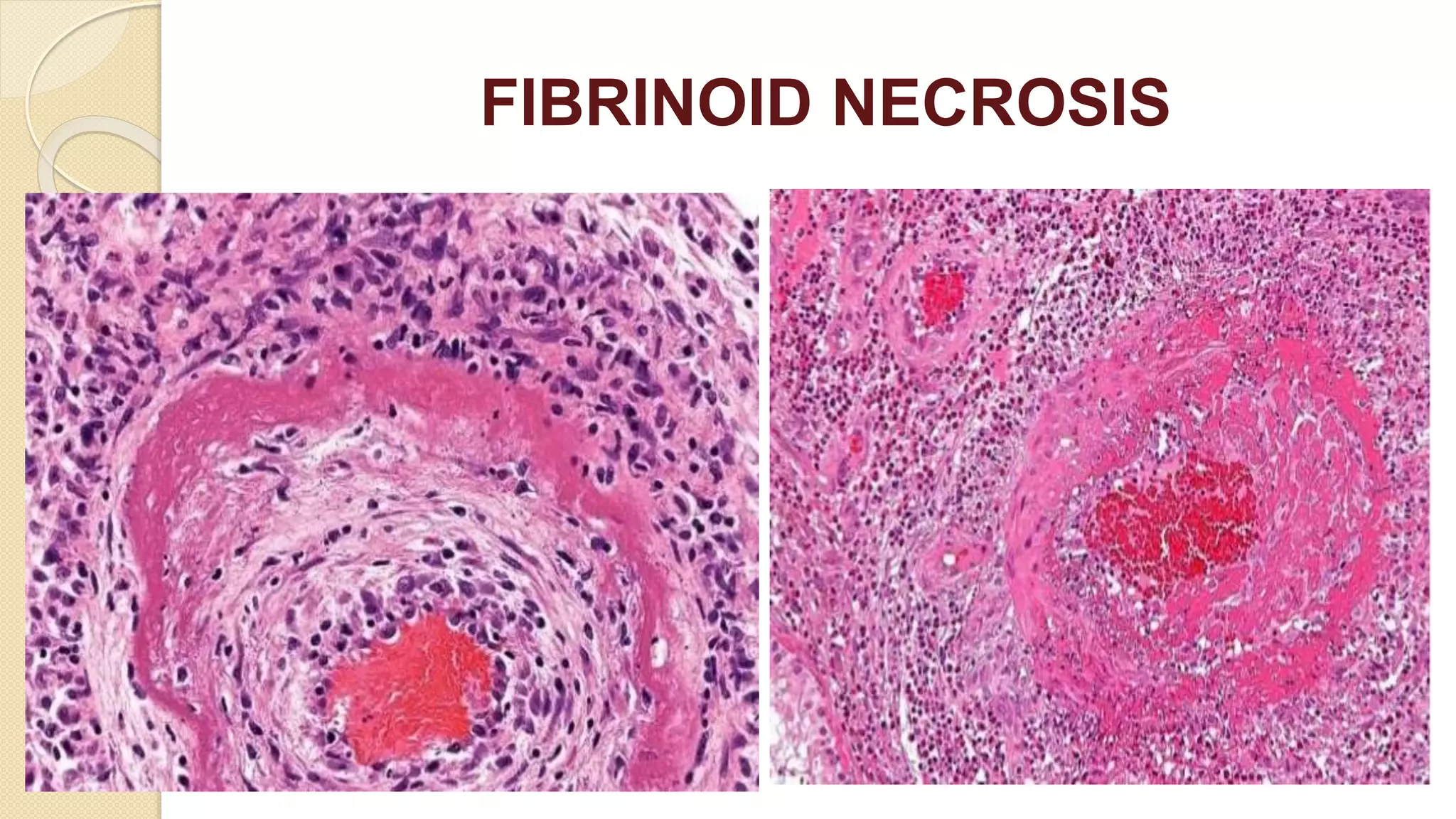
This document discusses necrosis, which refers to cell death and the subsequent morphological changes in tissues. There are several types of necrosis including coagulative, liquefactive, caseous, fat, and fibrinoid necrosis. Coagulative necrosis preserves the basic cell outline while liquefactive necrosis results in tissue liquefaction. Caseous necrosis is seen in tuberculosis and appears cheesy white. Fat necrosis results in calcium deposits in dead fat cells. Fibrinoid necrosis occurs when immune complexes are deposited in blood vessels. Microscopic examination reveals features of cytoplasmic and nuclear changes during necrosis.