Downloaded 604 times















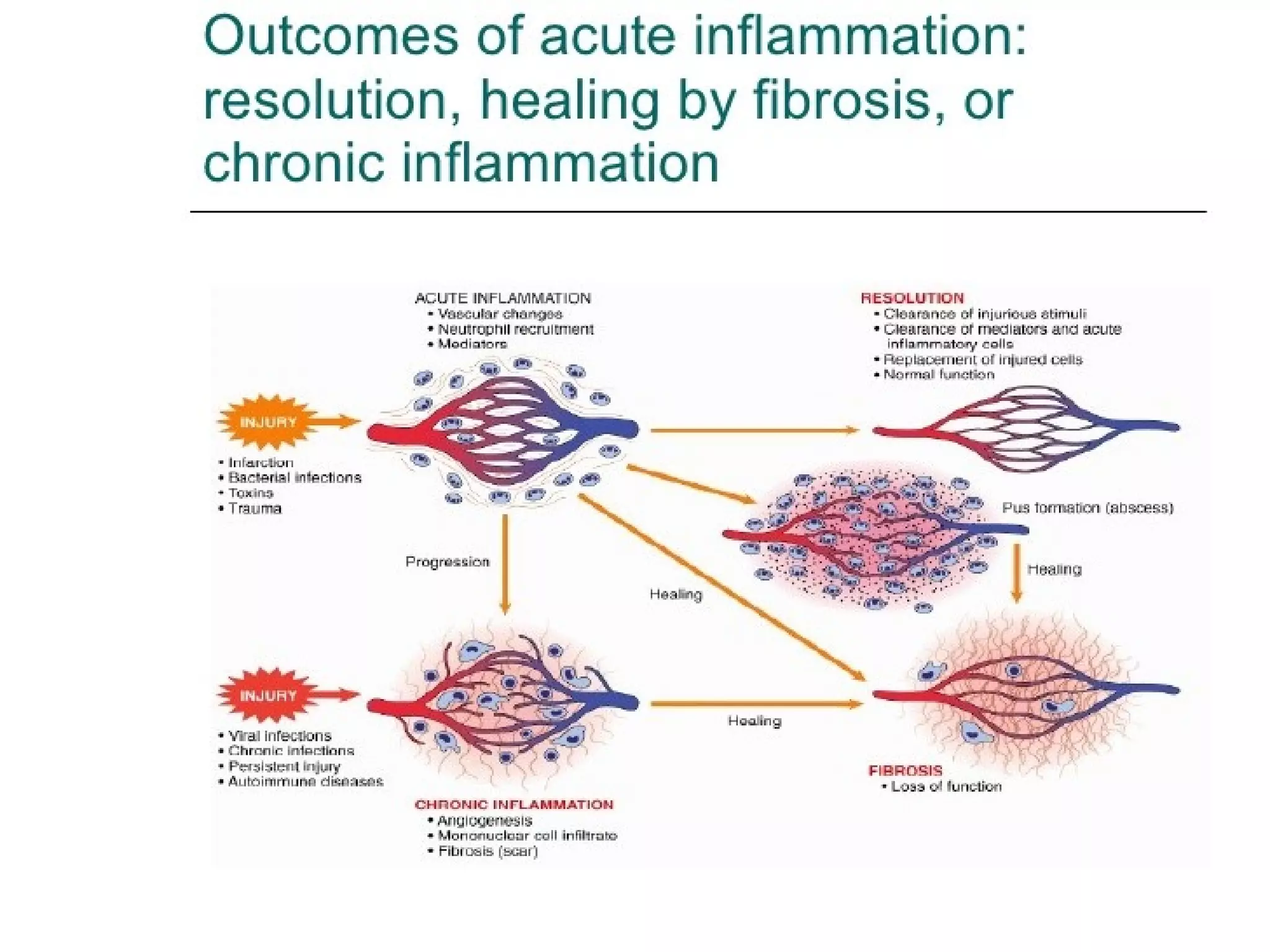













Acute inflammation is an immediate response to injury that involves increased blood flow, vascular permeability, and recruitment of leukocytes. This response aims to remove injurious stimuli and initiate tissue repair. It can resolve with complete healing or progress to chronic inflammation. Chronic inflammation is a prolonged response involving lymphocytes, macrophages and mediators that drives simultaneous tissue injury and repair through fibrosis. It underlies conditions like infection, autoimmunity and foreign body reactions. Systemic effects include fever, leukocytosis and acute phase responses.




































![Inflammation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/inflammationautosaved-180806124543-thumbnail.jpg?width=640&height=640&fit=bounds)


















































