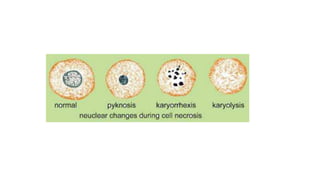
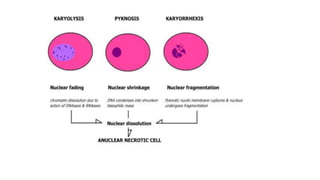
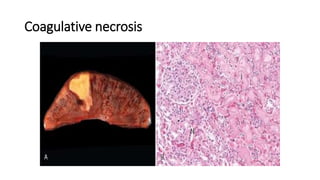
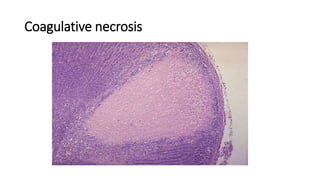
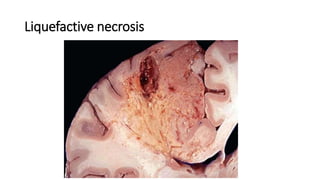
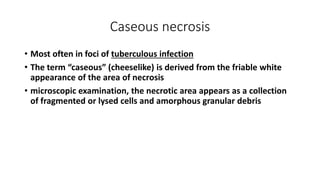
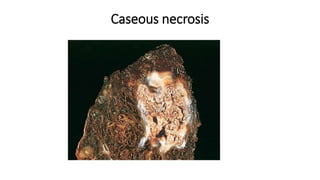
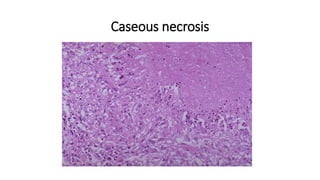
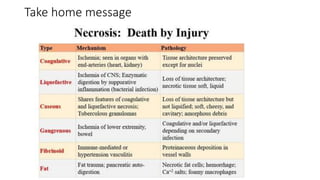
Necrosis is irreversible cell injury that can occur through several mechanisms and patterns. It involves severe damage to cell membranes leading to loss of integrity and contents leaking out. Morphological changes include nuclear changes like pyknosis, karyorrhexis, and karyolysis as well as cytoplasmic changes like dense eosinophilic cytoplasm and vacuolization. The main patterns discussed are coagulative necrosis, where architecture is preserved; liquefactive necrosis, where tissues digest into pus; and caseous necrosis, seen in tuberculosis as cheesy white areas.