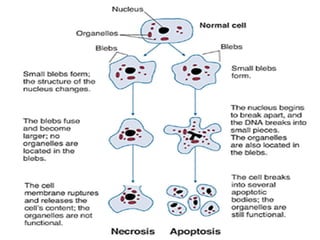
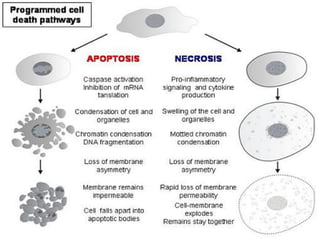
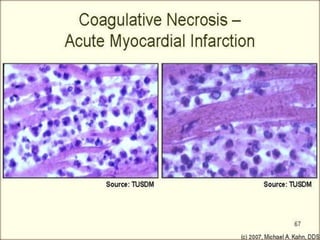
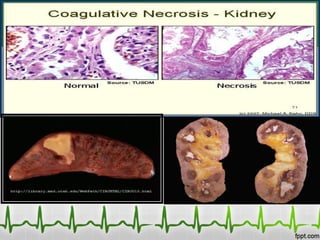
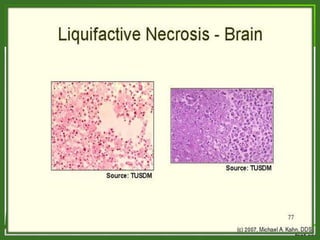
This document provides information on ischemia, necrosis, and their causes and types. It defines ischemia as insufficient blood supply causing oxygen and nutrient shortage. Causes include embolism, thrombosis, and aneurysm. Signs include tissue damage within minutes in highly aerobic tissues. Types are discussed like cardiac and limb ischemia. Necrosis is defined as cell death from loss of membrane integrity. Causes include anoxia, ischemia, chemicals and infections. Changes include cytoplasmic and nuclear changes. Necrotic cells may persist or be digested. Types discussed are coagulative, liquefactive, and caseous necrosis.