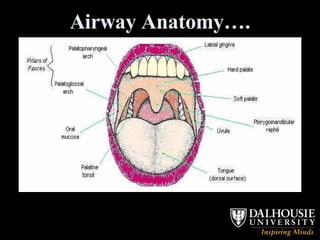
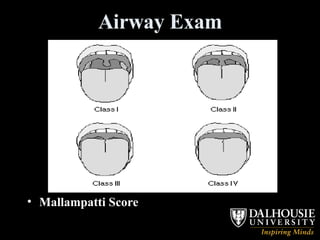
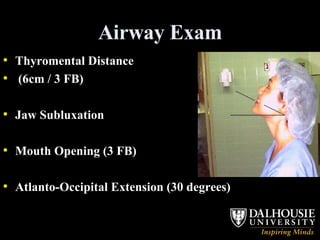
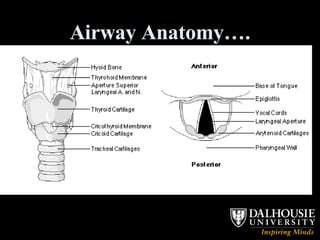
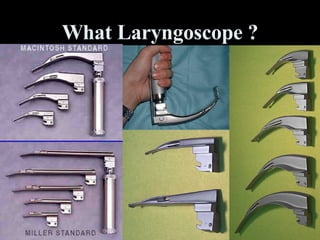
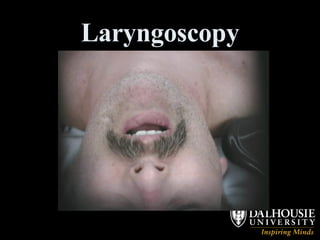
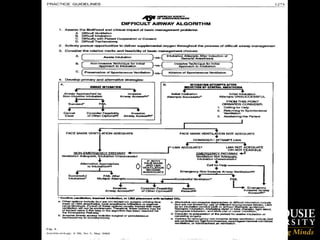
This document discusses airway management in the ICU for an obese patient with pneumonia who is deteriorating. It covers assessing the airway, sedation options like midazolam and fentanyl, difficult airway tools like bougies and LMAs, and special considerations for obese, rheumatoid arthritis, head/neck cancer, and trauma patients. The key is to oxygenate, assess ability to ventilate and intubate, call for help, and position the patient while preparing airway adjuncts and securing the airway.

























































![Anesthesia_for_Airway_management_and_Difficult_airway_Algorithmss[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiaforairwaymanagementanddifficultairwayalgorithmss11-250722203414-f94048f1-thumbnail.jpg?width=640&height=640&fit=bounds)


















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)




