Download to read offline

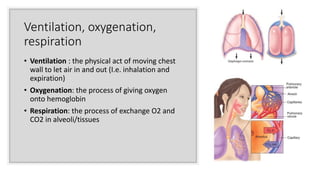
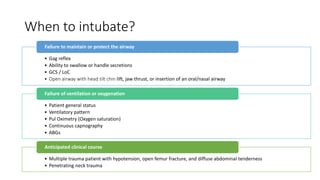
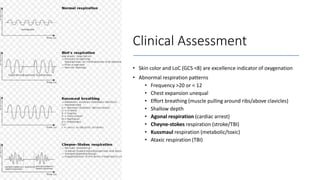
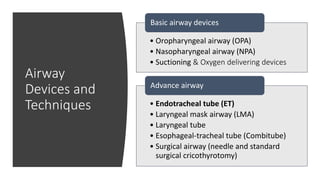

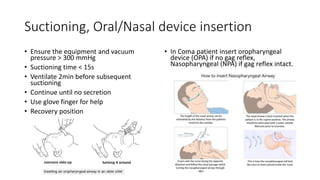

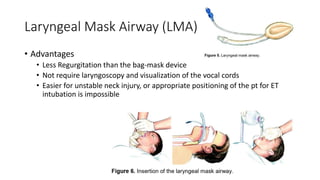

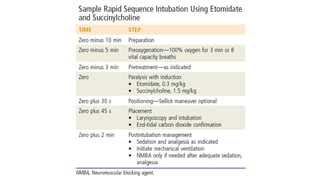
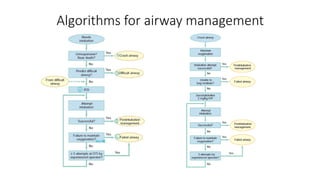
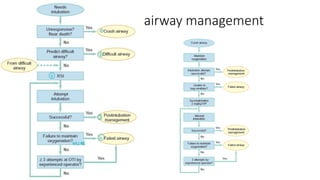
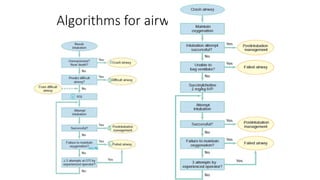
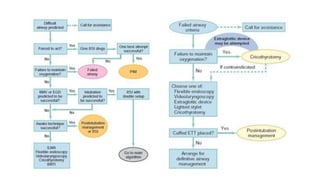

This document provides information on airway management techniques. It discusses: - The importance of airway management and oxygenation in resuscitation. - Clinical assessments for determining when to intubate a patient. - Basic and advanced airway devices like oropharyngeal airways, endotracheal tubes, and laryngeal mask airways. - Techniques for opening the airway like head tilt/chin lift and jaw thrust maneuvers. - Methods for intubation including rapid sequence intubation and its components. - Approaches for difficult airways including video laryngoscopy and rescue techniques if intubation fails.












































![Anesthesia_for_Airway_management_and_Difficult_airway_Algorithmss[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/anesthesiaforairwaymanagementanddifficultairwayalgorithmss11-250722203414-f94048f1-thumbnail.jpg?width=640&height=640&fit=bounds)











![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)








![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

