Downloaded 212 times


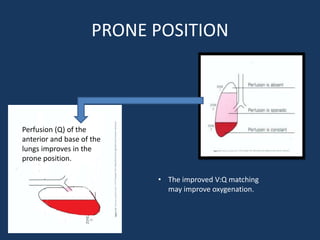
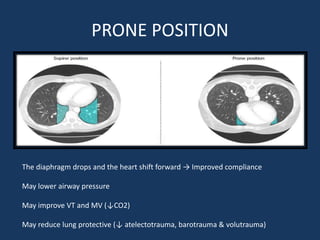


The document discusses the prone position as a rescue therapy for severe Acute Respiratory Distress Syndrome (ARDS), characterized by acute lung inflammation and impaired oxygenation. It outlines the stages and severity classification of ARDS, treatment approaches, indications and contraindications for prone positioning, and its benefits for improving lung function and oxygenation. Current research supports its use within the first 48 hours of ARDS onset, with recommended durations of 12-24 hours for optimal effectiveness.






















































































