Downloaded 278 times





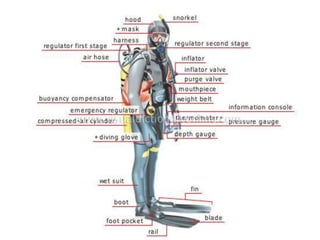








The document provides a comprehensive overview of scuba diving, including its history, equipment, gas laws, and potential pathologies resulting from diving injuries. It highlights key conditions such as barotrauma and decompression sickness, detailing clinical manifestations and treatment options, particularly the use of hyperbaric oxygen therapy. Overall, it emphasizes the increasing popularity of recreational diving and the importance of understanding associated risks and emergency management.



























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














