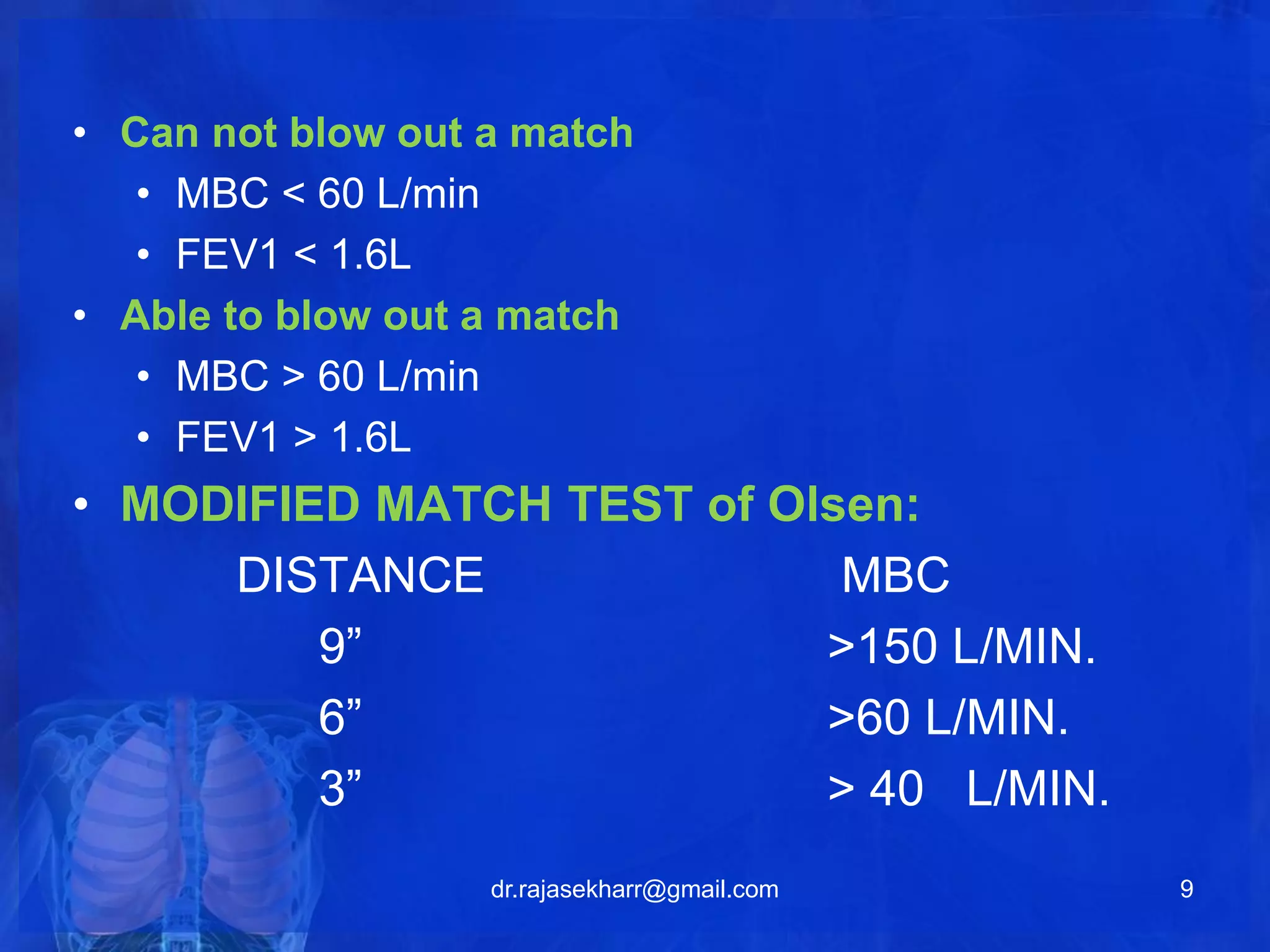
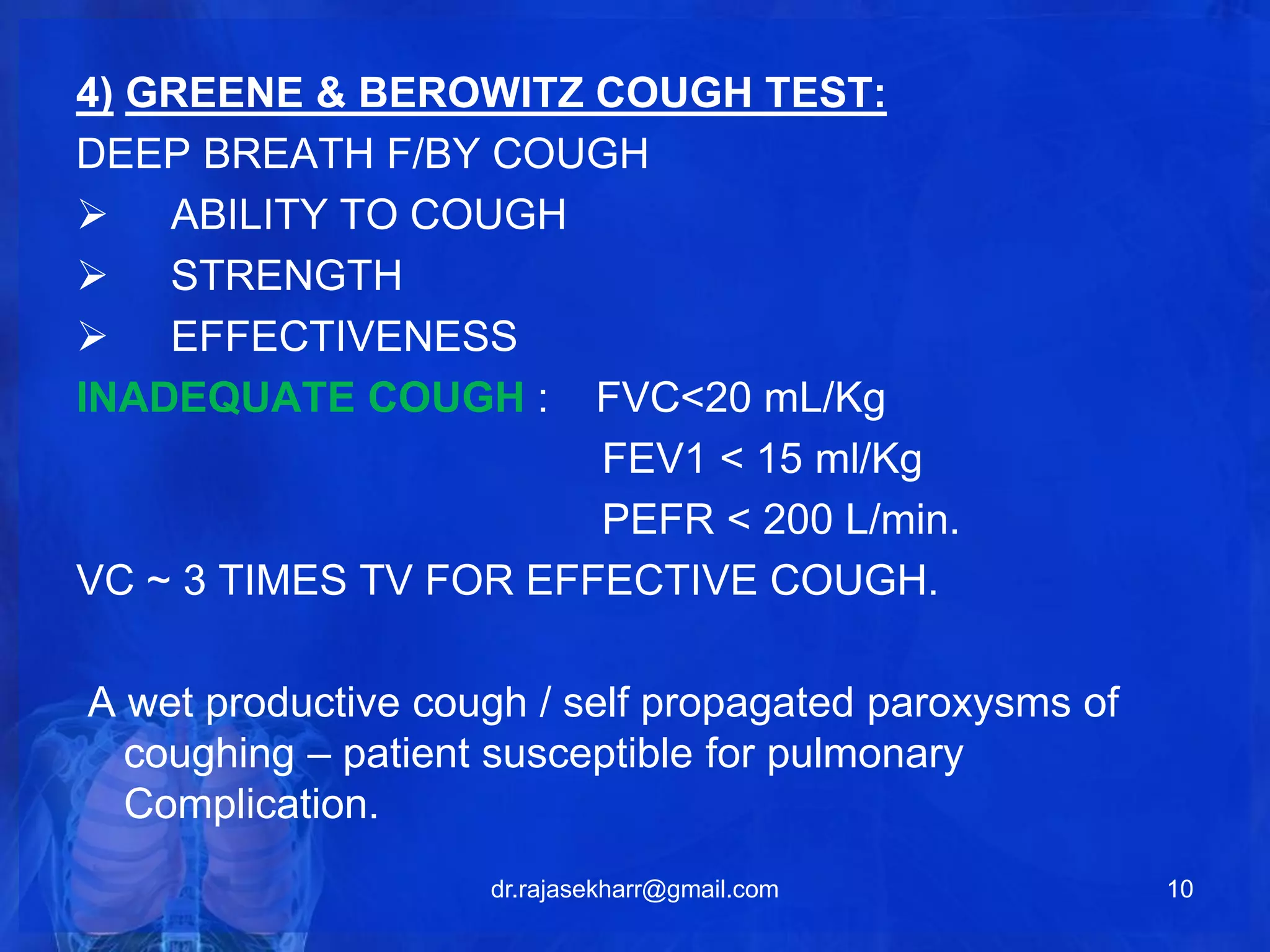
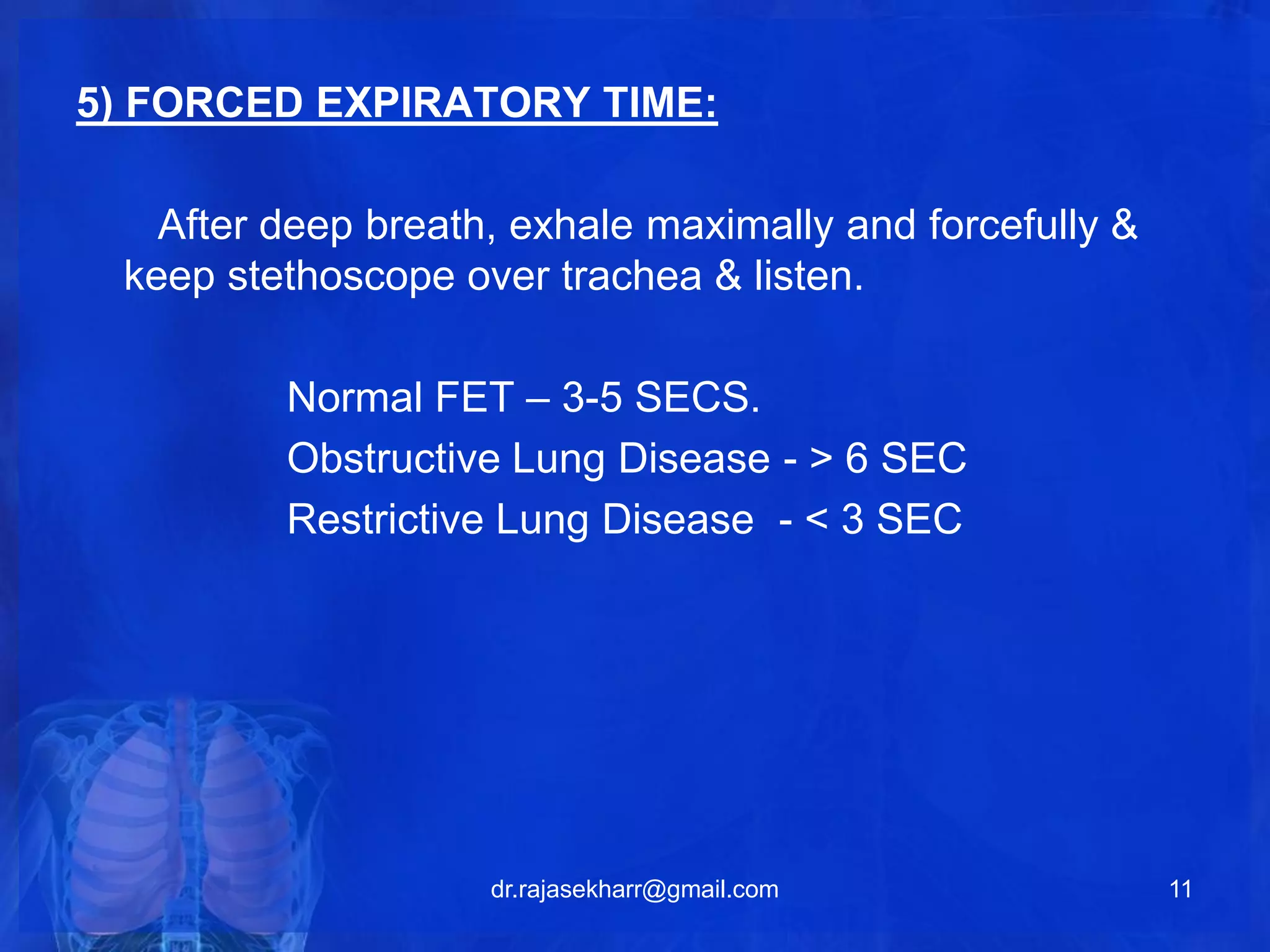
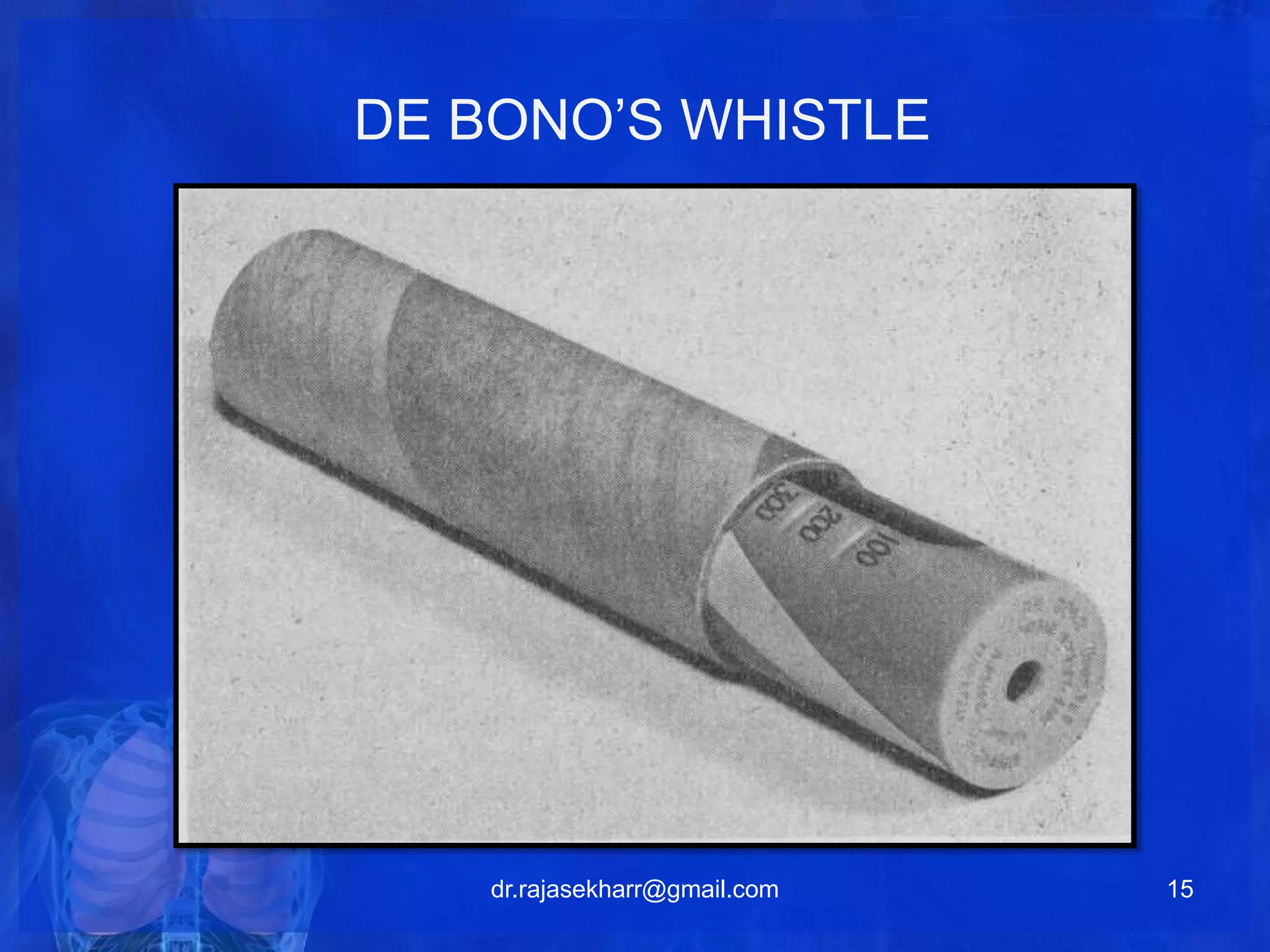
The document describes various bedside pulmonary function tests that can be used to assess lung function and predict postoperative risk. Some of the tests described include the breath holding test to measure cardiopulmonary reserve, single breath count to measure vital capacity, match blowing test to measure maximum breathing capacity, cough test to evaluate cough strength, and tests using a respirometer or whistle to measure parameters like peak expiratory flow rate. The tests provide information on lung volumes, flows, and ability that can help identify patients at risk for pulmonary complications during or after surgery.