Downloaded 1,144 times

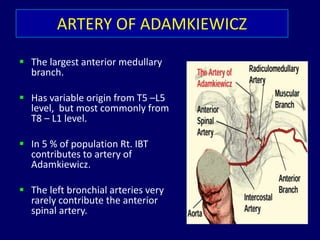
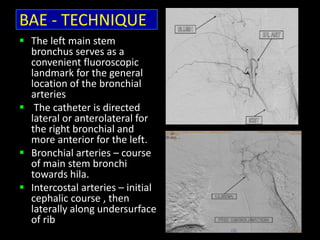
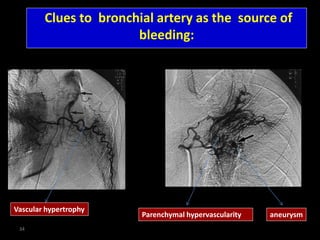
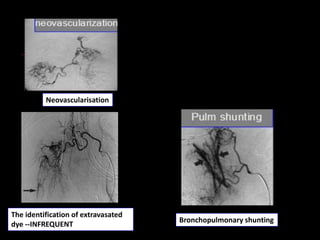
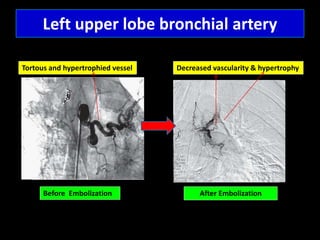
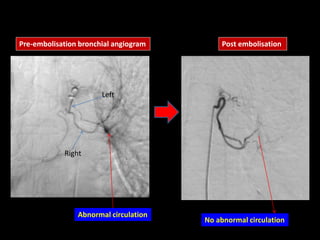
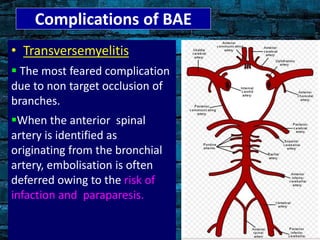


Bronchial artery embolization (BAE) is a minimally invasive procedure used to control massive or recurrent hemoptysis by occluding the blood supply to the lungs via selective catheterization and embolization of abnormal bronchial vessels. BAE has a high rate of immediate bleeding control of 57-100% and long-term control of 70-88%. Potential complications include tissue infarction if smaller embolic particles are used and transverse myelitis if branches supplying the spinal cord are inadvertently occluded. Careful angiography is required to identify the origin of vessels like the artery of Adamkiewicz to avoid neurologic complications during the procedure.































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)
![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)










