This document provides information about drowning, including:
1. The mechanisms, morphological features, and differences between freshwater and saltwater drowning.
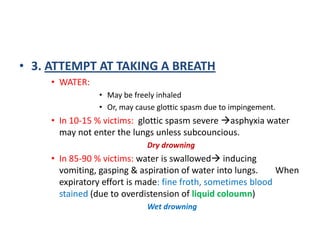
2. The sequence of events in drowning including panic, voluntary apnea, attempts to breathe water, and cessation of struggling.
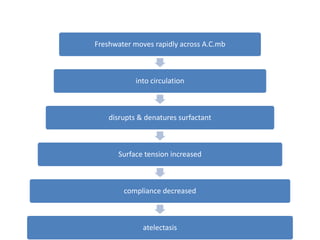
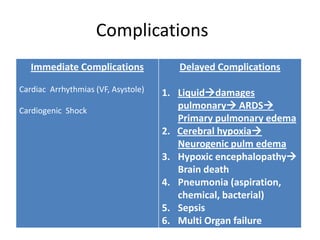
3. Pathophysiological effects of freshwater and saltwater drowning on organs like the lungs, heart, and brain.
4. Macroscopic findings commonly seen in drowning such as lung edema, foam in airways, and skin and muscle hemorrhages.
5. Diagnostic tests and the timeline for resuscitation efforts in drowning victims.