Downloaded 136 times
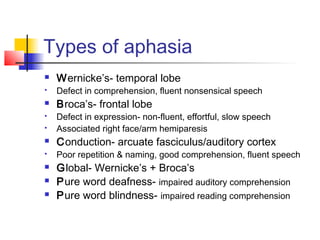

This document discusses disorders of higher mental functions including amnesia, aphasia, apraxia, agnosia, delirium, and dementia. It provides details on the lateralization of brain function between the left and right hemispheres. Specific types of amnesia, aphasia, apraxia, and agnosia are defined along with their causes and characteristics. Delirium and dementia are also described, including their presentations, causes, and management approaches.



















































![DELIRIUM_&_DEMENTIA[1]_Ngoma.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/deliriumdementia1ngoma-231022110253-0a2f4eb8-thumbnail.jpg?width=640&height=640&fit=bounds)

































