Downloaded 114 times
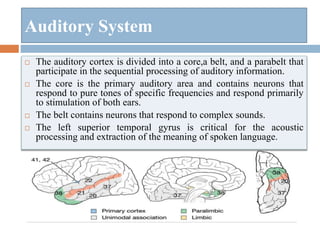
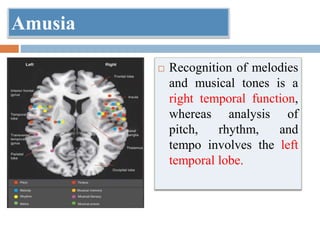
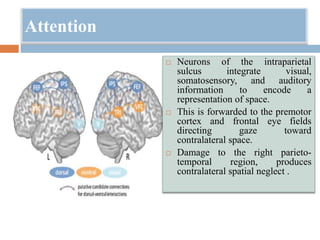
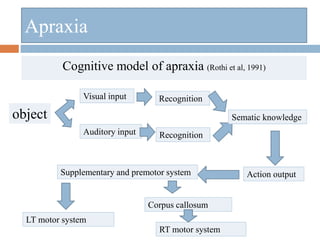
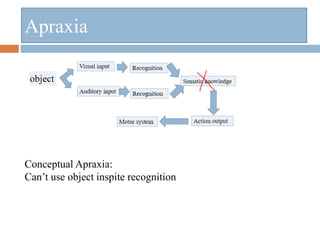
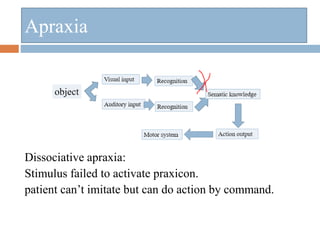
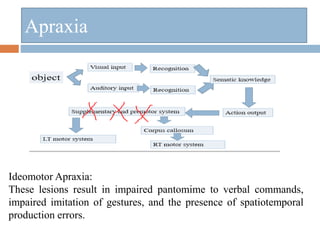
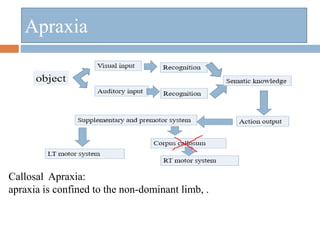

This document summarizes higher cortical functions including language, calculations, spatial awareness, memory, executive function, music and creativity. It discusses the cerebral cortex and different types of association cortices. It then examines various neurological functions like sensory processing, attention, motor programming, language, memory, agnosias, apraxia, aphasia and alexia. Key areas discussed include the visual and auditory systems, object recognition networks, spatial attention, praxis, types of agnosia and aphasia, and the neuroanatomy underlying different language functions.
















































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





