Downloaded 26 times
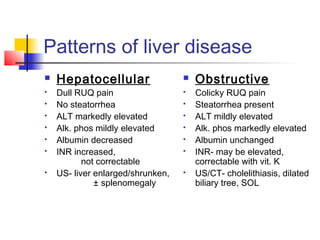

This document discusses liver function tests and how to evaluate liver disease patterns. It outlines the clinical presentation of hepatocellular and cholestatic liver disease. Key investigations covered include liver enzymes, bilirubin, albumin, clotting factors and their significance. Imaging modalities like ultrasound, CT and MRI are also mentioned. The patterns of hepatocellular vs obstructive liver disease are compared in terms of symptoms, enzyme levels and imaging findings.























































































