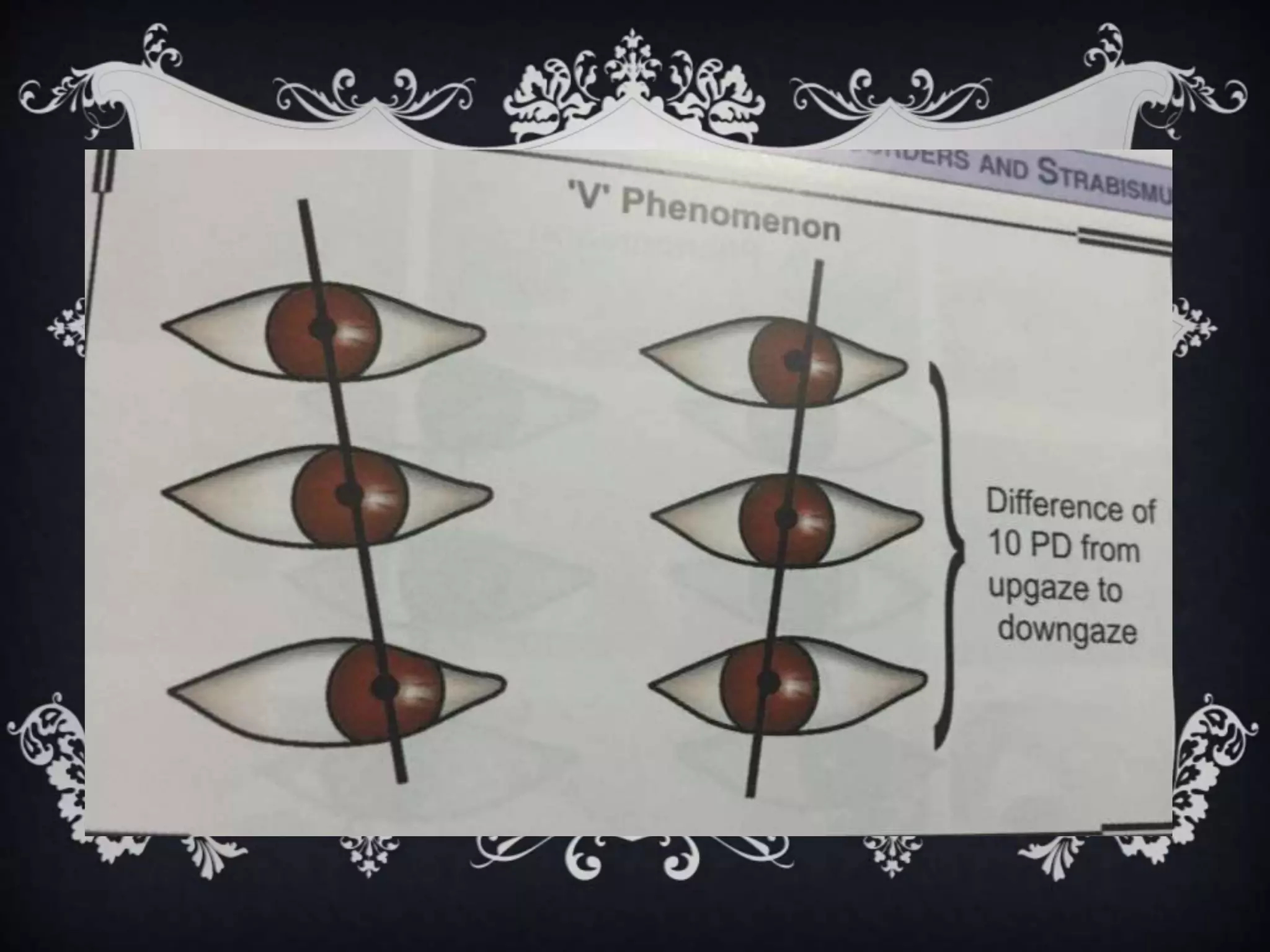
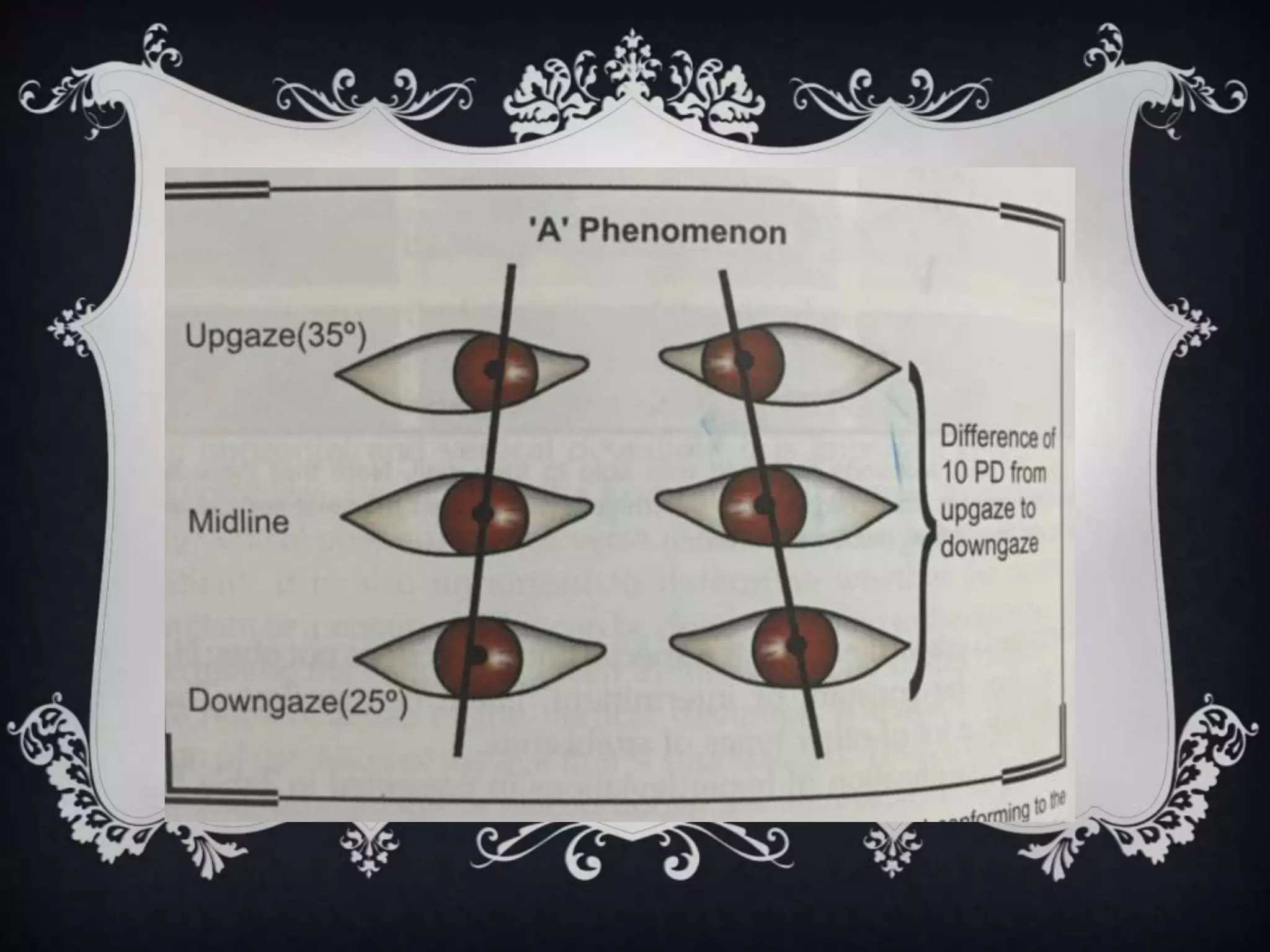
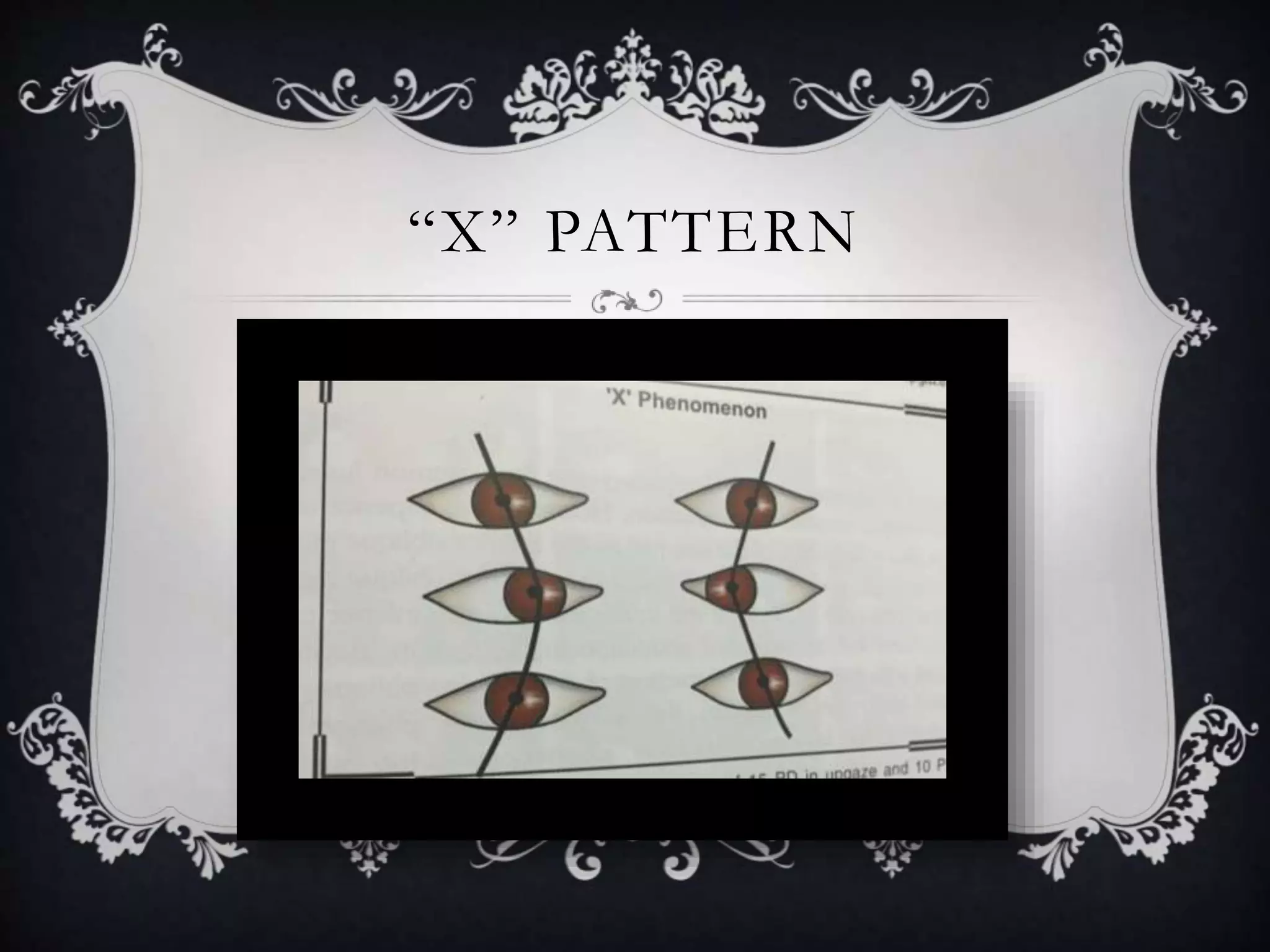
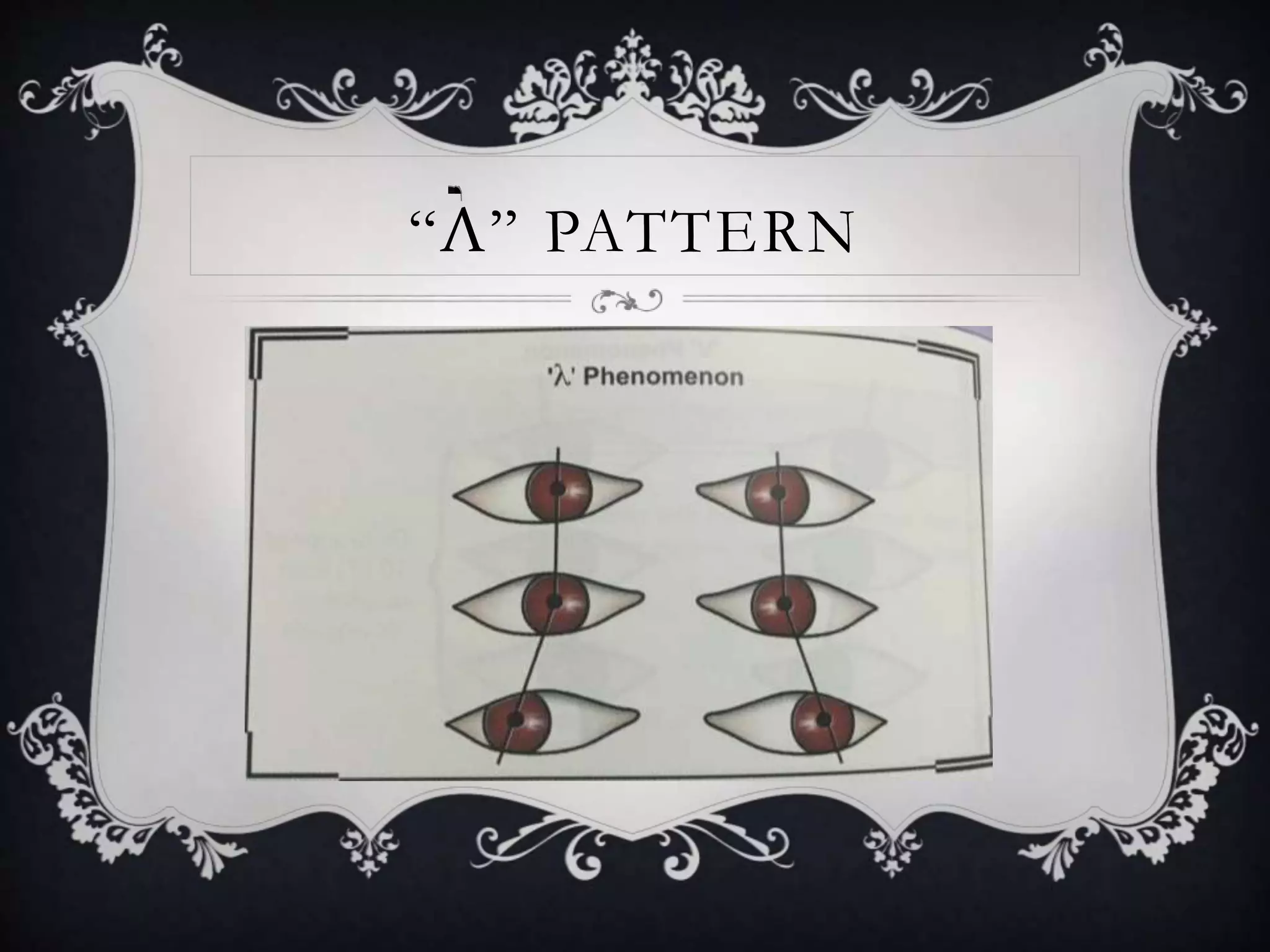
Cyclovertical anomalies refer to vertical deviations of the eyes involving the cyclovertical muscles. There are various types including comitant and incomitant vertical deviations. Patterns of strabismus like V, A, X, Y patterns are classified based on how the horizontal deviation changes between upgaze and downgaze. Conditions like superior oblique overaction, palsy, inferior oblique overaction are described. Dissociated vertical deviation is an innervational disorder seen in infantile strabismus and involves predominately vertical movements of one eye drifting upward and outward. Surgical management of these conditions aims to weaken muscles or transpose them.