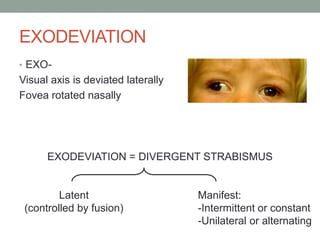
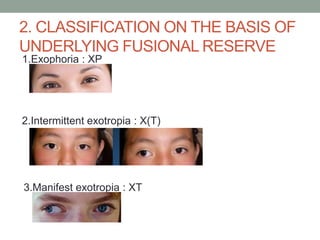
1. Exodeviations, or divergent strabismus, involve lateral deviation of the visual axis and nasal rotation of the fovea. The main types are exophoria, intermittent exotropia, and manifest exotropia.
2. Causes of exodeviations include excessive tonic divergence, anatomical factors in the orbit, and high accommodative convergence to accommodation ratio.
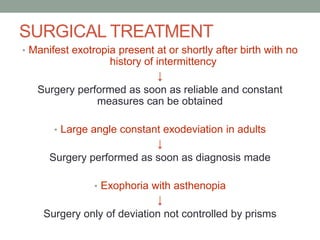
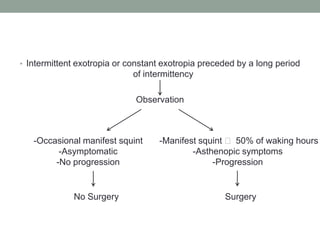
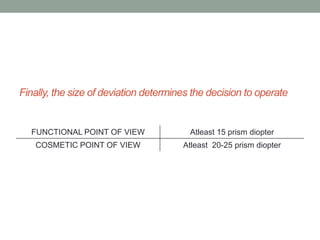
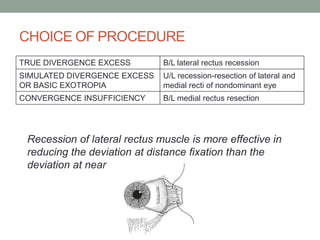
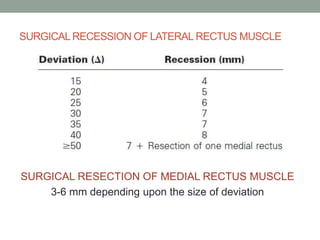
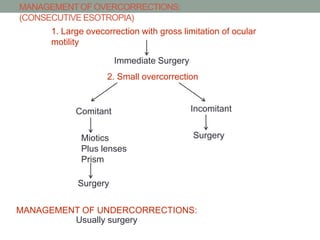
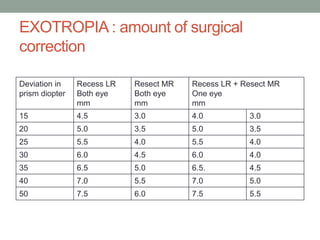
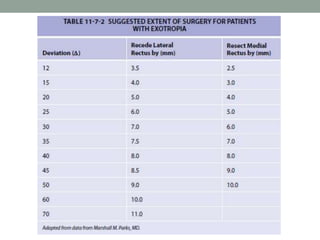
3. Treatment involves correcting refractive errors and amblyopia non-surgically and recessing the lateral rectus or resecting the medial rectus surgically depending on the type and amount of deviation. The goal of surgery is a small overcorrection to stabilize binocular alignment.