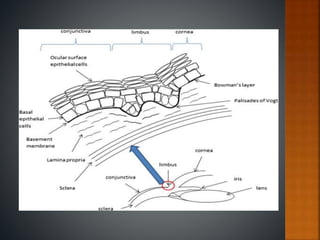
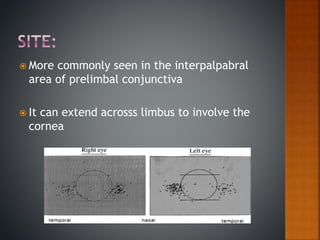
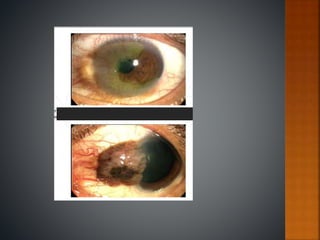
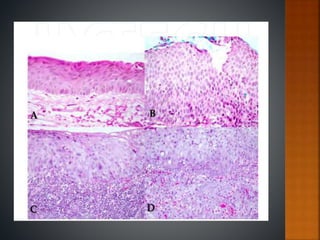
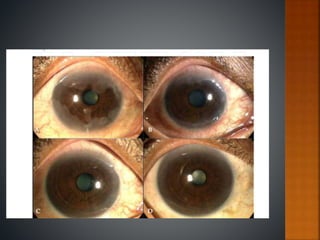
Ocular surface squamous neoplasia (OSSN) is a spectrum of neoplasms originating from squamous epithelium of the conjunctiva, limbus, and cornea. Risk factors include UV radiation exposure, HPV infection, immunosuppression, and HIV infection. Clinically, OSSN presents as an elevated fleshy lesion near the limbus. Diagnosis is confirmed by biopsy and histopathology. Treatment involves complete surgical excision with cryotherapy or topical chemotherapy as adjuvant therapy. Prognosis is generally good with modern treatments and local recurrence rates below 5%.