This document summarizes the basics of pediatric refraction as presented by Dr. Mahamud Adnan. Key points include:
1) Pediatric refraction requires great expertise as it is different from normal refraction due to active accommodation in children. Cycloplegic refraction is preferable to paralyze the ciliary muscles.
2) The refractive status of infants and children changes rapidly in the first year as visual development occurs. Cycloplegia allows determining the true refractive error without accommodation.
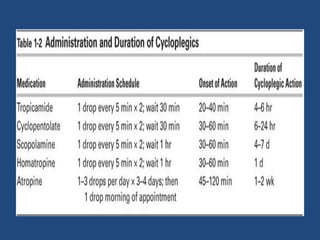
3) Cycloplegic drugs like atropine and cyclopentolate are used which have side effects like blurred vision but allow full paralysis of accommodation for accurate refraction assessment. Timely intervention and




























![Optics of contact lens and nomenclature copy [repaired] (1)](https://cdn.slidesharecdn.com/ss_thumbnails/opticsofcontactlensandnomenclature-copyrepaired1-170218054900-thumbnail.jpg?width=640&height=640&fit=bounds)















































