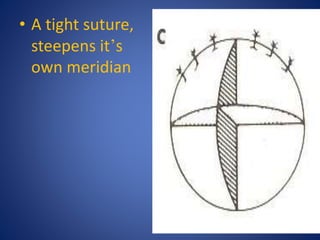
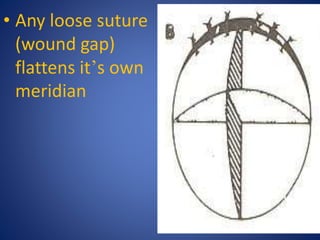
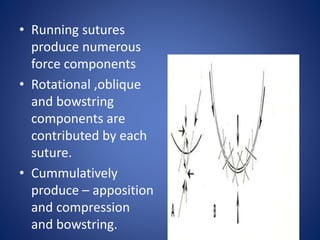
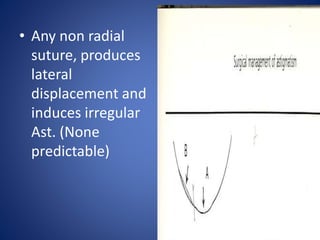
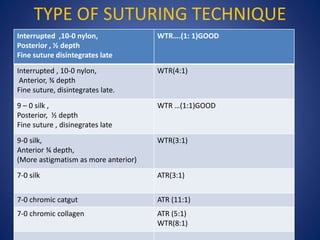
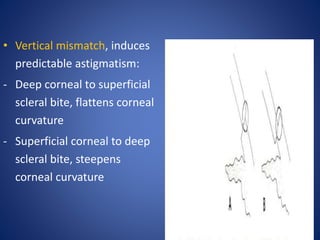
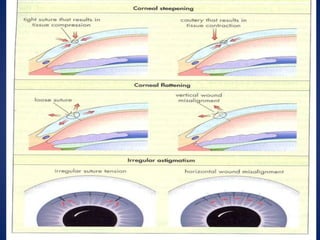
This document discusses sources and management of postoperative astigmatism after cataract surgery. It notes that the main sources of astigmatism are preexisting astigmatism, incision characteristics like length and location, and suture characteristics like type, tension, and placement. Larger or superior incisions, and sutures that degrade quickly or are placed unevenly, tend to cause more astigmatism. Managing factors like smaller incisions, frown-shape cuts, posterior placement, uniform tension, and non-degrading suture material can help minimize postoperative astigmatism. Precise suture removal timing and selective cutting can further refine astigmatism outcomes after surgery.






















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)



