Downloaded 18 times






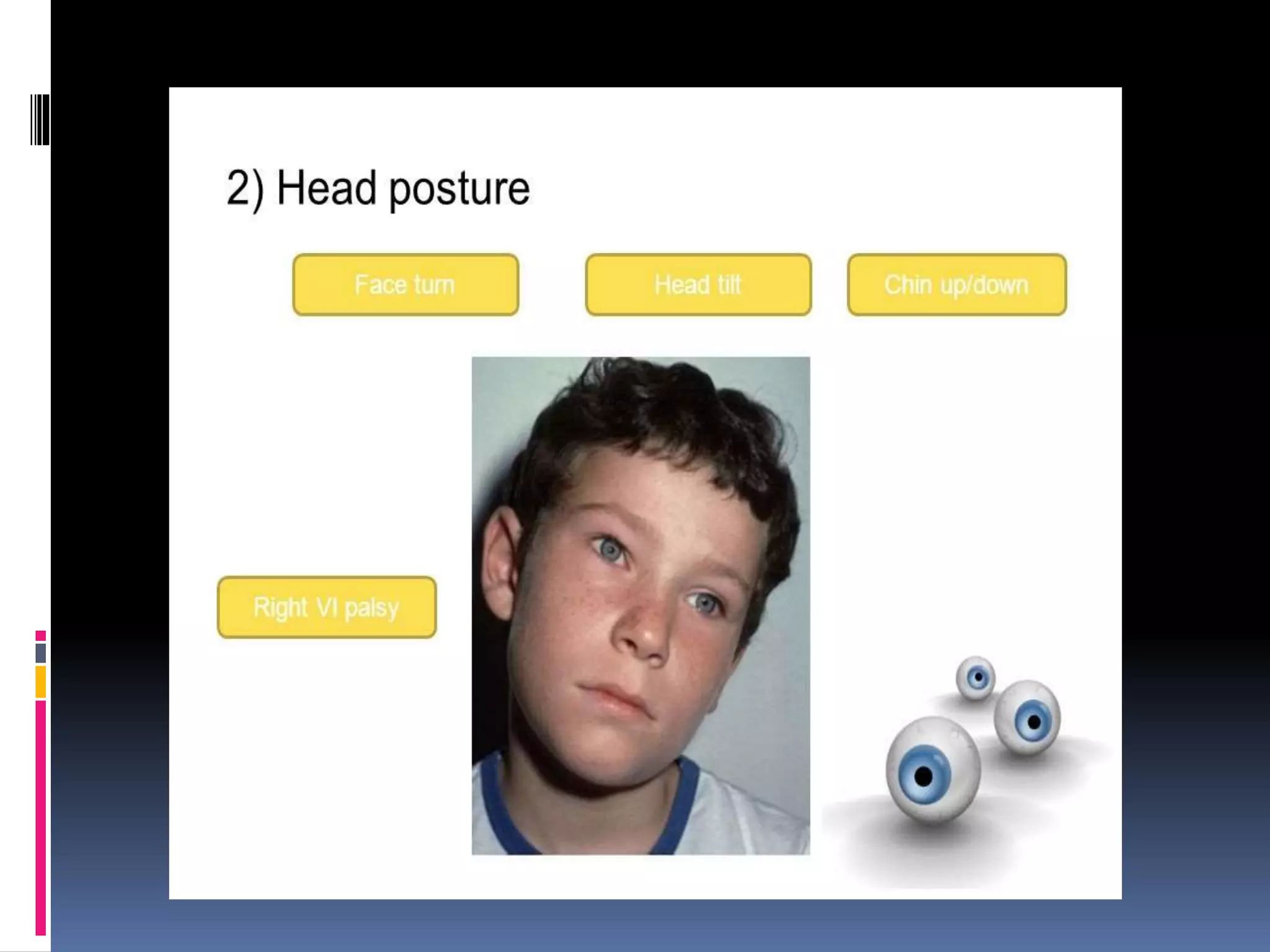







This document outlines the order and components of a general orthoptic examination. The examination aims to diagnose ocular motor disorders and detect other eye or non-eye issues. It involves assessing appearance, measuring visual acuity, observing eyelids and eye position, and measuring eye movements and deviations. It also includes refraction with cycloplegia, investigating binocular function, and potential laboratory/radiology tests. Specific examination points cover general appearance, head posture, eyelid assessment, ocular deviation and movement testing, and evaluating binocular visual functions.












































































