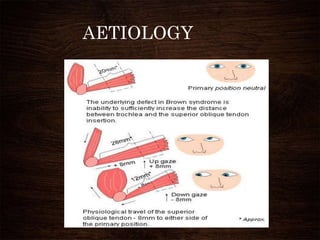
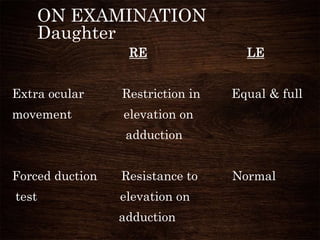
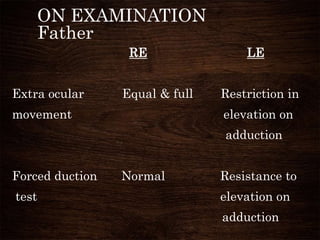
Brown syndrome is a congenital restrictive strabismus disorder characterized by limited elevation of the eye in adduction. It is caused by anatomical abnormalities of the superior oblique tendon that restrict its movement. Clinical features include inability to elevate the eye in adduction and resistance to elevation on forced duction testing in adduction. Diagnosis is based on these clinical exam findings. Treatment options aim to surgically release the restriction, such as complete tenectomy or tendon expanders, depending on the severity of symptoms.













![Types of pediatric contact lens [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/typesofpediatriccontactlensautosaved-200210123904-thumbnail.jpg?width=640&height=640&fit=bounds)













































































