Downloaded 328 times



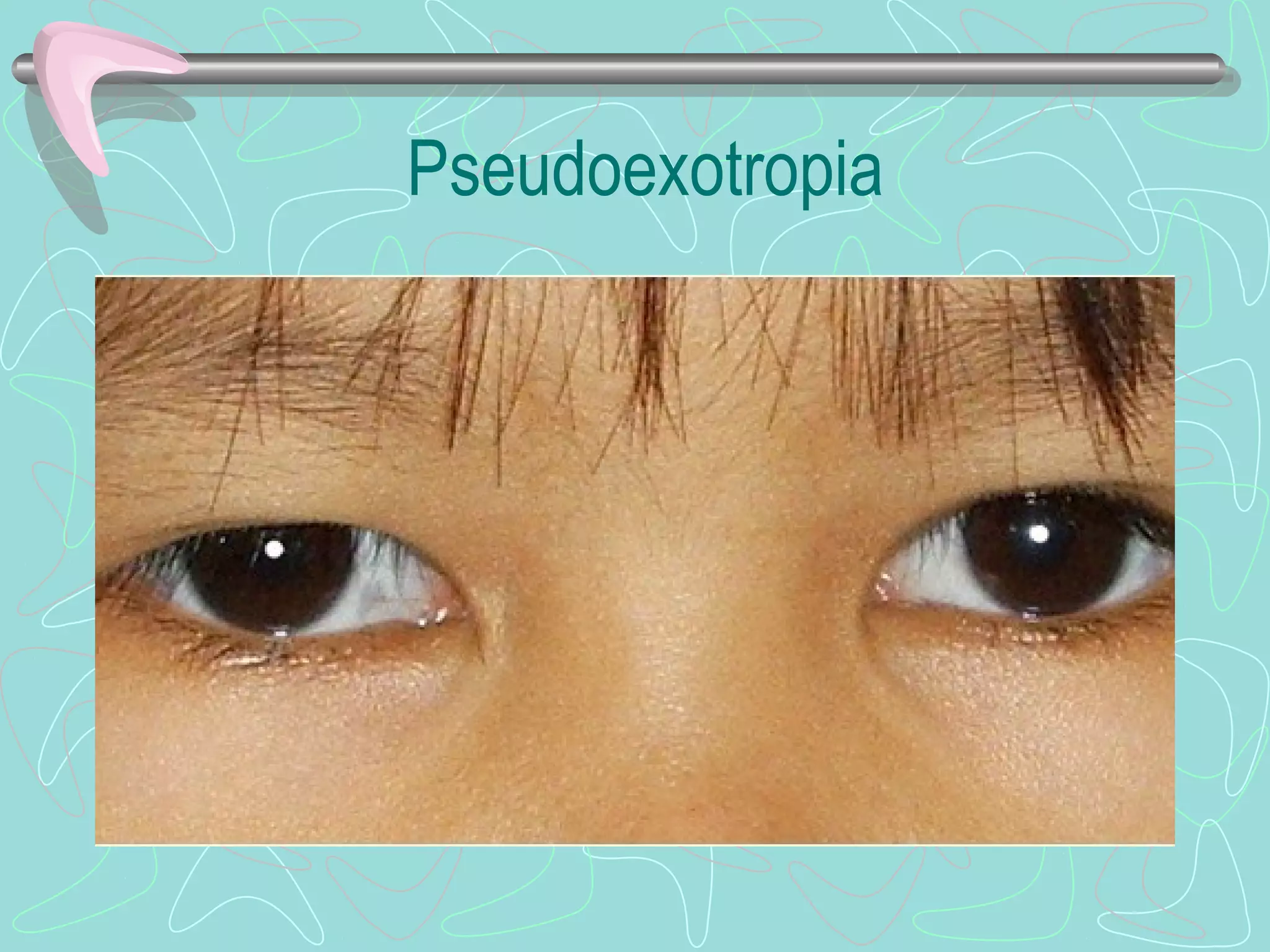

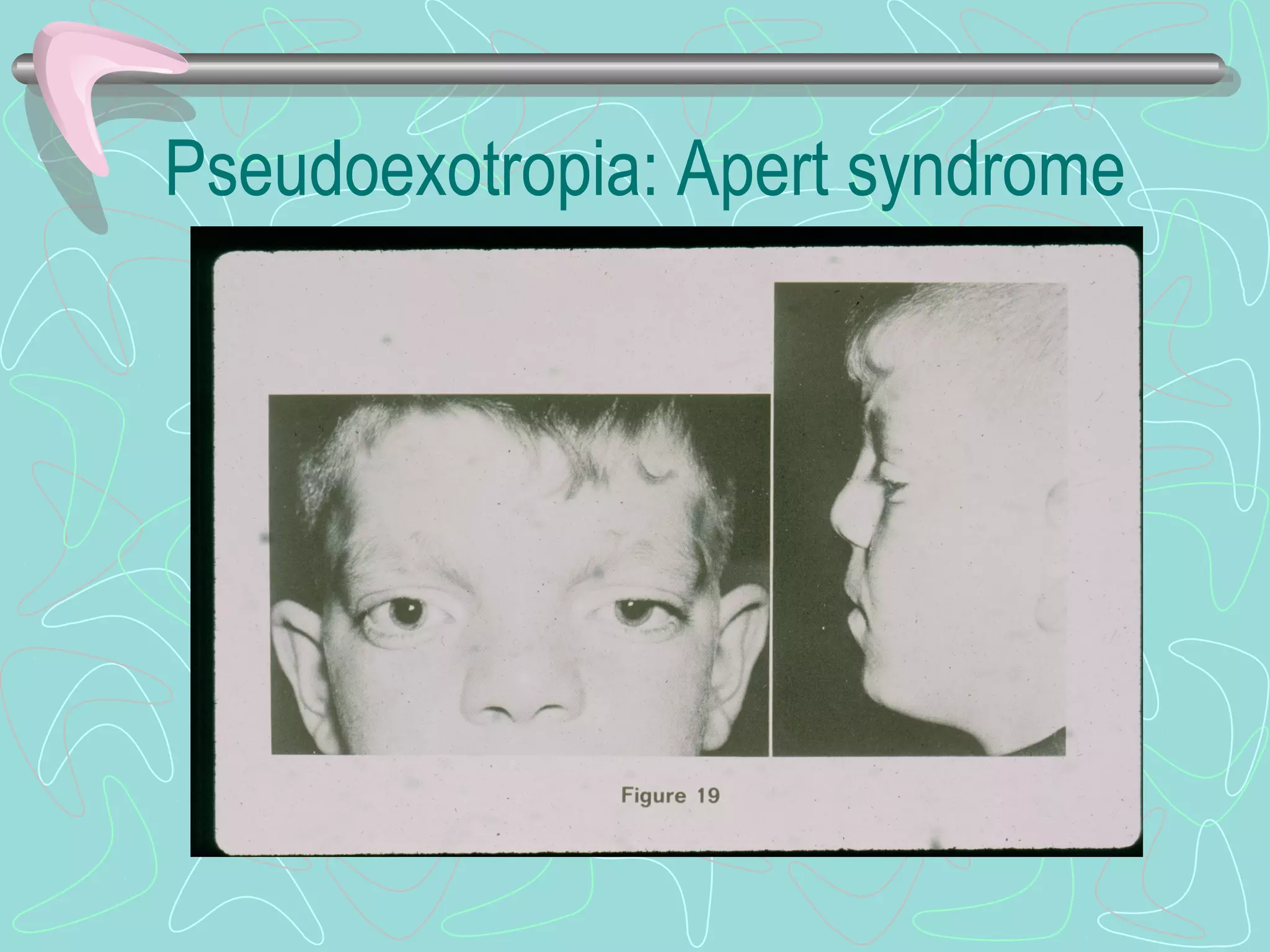

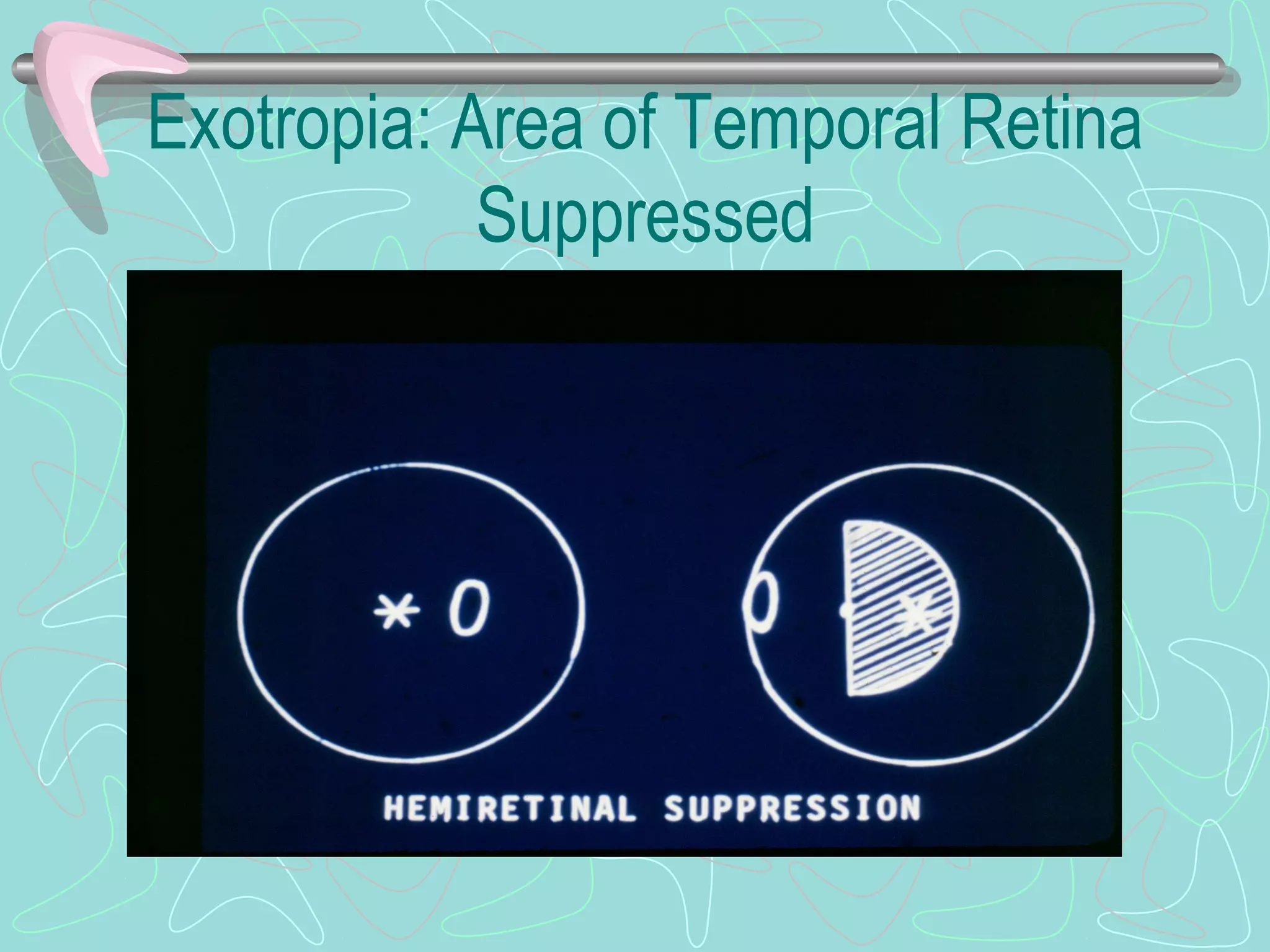

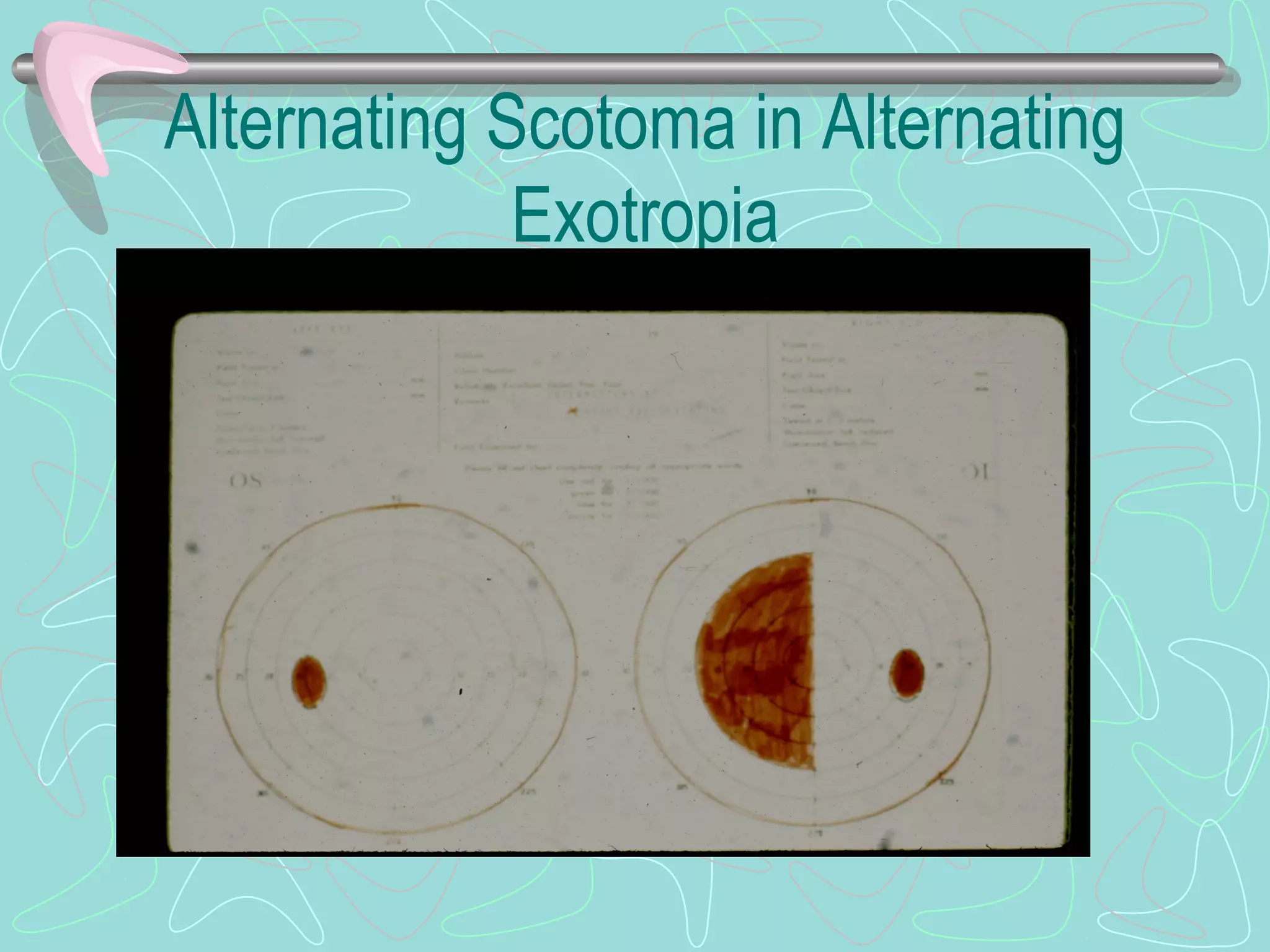

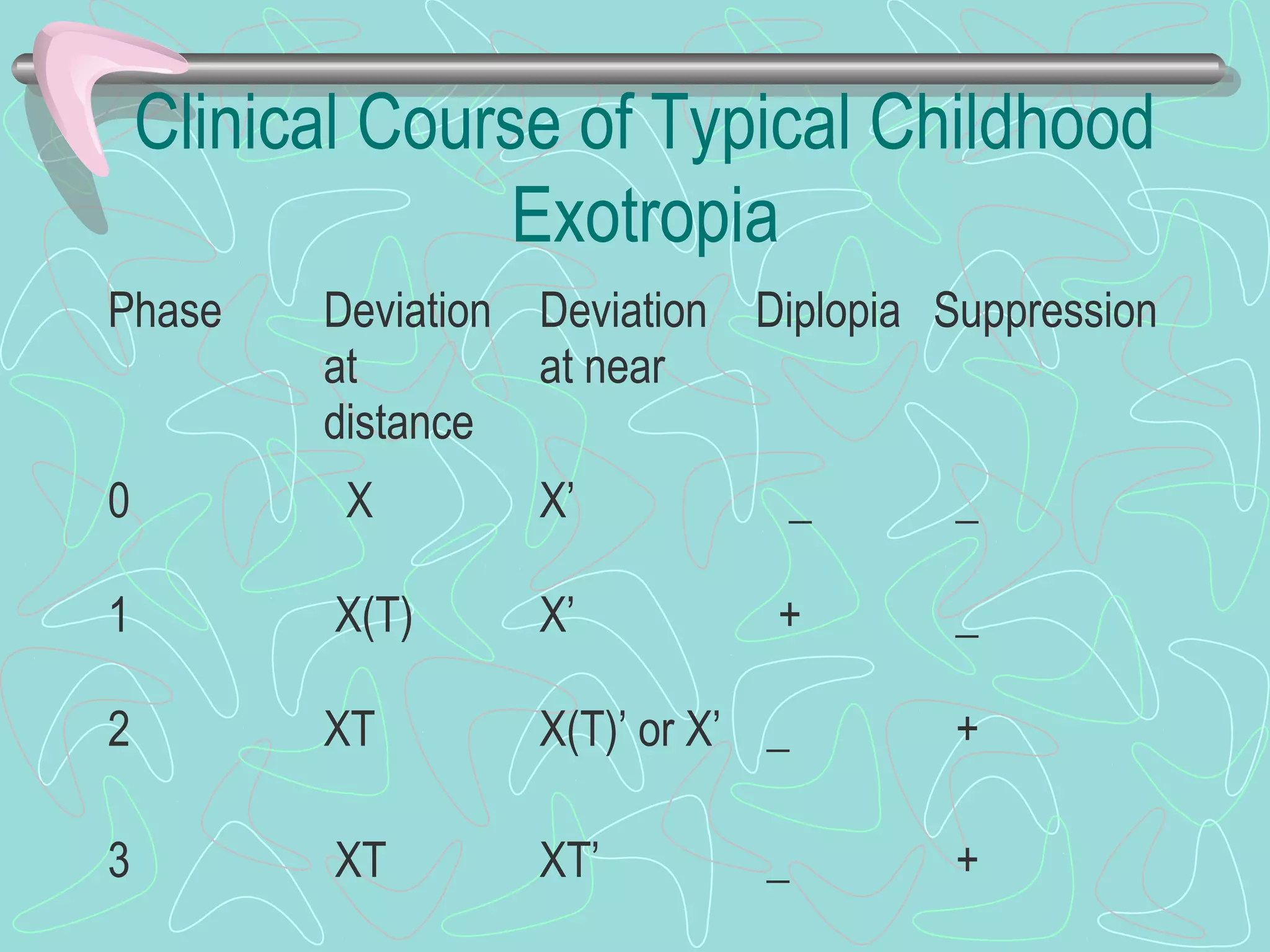








Exotropia is an eye condition where the eyes turn outward. There are several types of exotropia including congenital, sensory, typical childhood, and convergence insufficiency. Exotropia is classified based on fusion status and the AC/A ratio. Treatment involves maximizing vision, glasses, patching, prisms, or surgery. Surgery typically involves recessing the lateral rectus muscles and may also include recessing or resecting the medial rectus muscles. The goal of surgery is to achieve a small angle of esotropia initially to prevent overcorrection and recurrence of exotropia.























































































