The document appears to be incomplete or not available for summarization. No information could be extracted to create a meaningful summary. Please provide a complete document for summarization.
Optom. Ankit S.Varshney
B.Optom, M.Optom, Ph.D. in Optometry (pursuing) Fellow of IACLE (Aus.), Fellow of ASCO(Mum.)
Prof. at (Shree Bharatimaiya College of Optometry & Physiotherapy, Surat)
Life Member of Indian Optometric Association (IOA)
Associate Member of Association of Schools and Colleges of Optometry(ASCO)
Member of Optometry Council of India(OCI)
Educator Member of International Association of Contact lense Educators (Australia)(IACLE)
Mail id: ankitsvarshney@yahoo.com
Whatsapp no. +918155955820
ALPHABETICAL PATTERN
Vertically incomitant
Horizontally comitant deviation
2.
References
BINOCULAR VISION& STRABISMUS –GK VON NOORDEN
CLINICAL MANGEMENT OF STRABISMUS ELEZABETH
E.CALAROSSA & MICHAEL W. ROUSE
AAO- SECTION: PEDIATRIC OPHTHALMOLOGY &
STRABISMUS
STRABISMUS SIMPLIFIED- PRADEEP SHARMA
PRACTICAL ORTHOPTICS IN THE TREATMENT OF SQUINT-
LYLE AND JACKSON’S
7/15/2020Optom. Ankit varshney2
3.
Types of strabismus
1. Apparent/ Pseudo Strabismus: nothing but an optical
illusion caused by prominent epicanthal folds (pseudo eso)/
wide IPD (pseudo exo).
2. Latent Strabismus (Phoria): deviations are present only
some of the time: (interruption of BV, fatigue, illness,
stress)
3. Manifest Strabismus (tropia): eyes deviated all the time
Concomitant ( Non-paralytic)
Incomitant strabismus: Manifest squint in which the
amount of deviation varies in different directions of gaze. 7/15/2020Optom. Ankit varshney3
4.
A-V pattern
Itdenotes the fact that there is a
considerable difference in the angle of
horizontal deviation on looking upward as
compared with looking downwards.
It can be exodeviations or esodeviations
that measure differently in upgaze, primary
position and downgaze.
As the eyes move from upgaze to
downgaze, instead of making parallel
upward and downward movements, the
eyes move up and down in particular
pattern.
This pattern can have the configuration of
A, V, X, Y,◊ or .
7/15/2020Optom. Ankit varshney4
5.
TYPES
1) A-pattern :-
“A” phenomenon in ESOphoria
and ESOtropia:- On looking
directly upwards, the convergent
deviation is considerably greater
than when looking directly
downwards.
“A” phenomenon in EXOphoria
and EXOtropia:- On looking
directly downwards the divergent
deviation is considerably greater
than when looking upwards.
Eso ↑ Upgaze
Exo ↑ Downgaze 7/15/2020Optom. Ankit varshney5
6.
“A”phenomenon
The termapplied to those cases which show a
considerable increase in the angle of
convergence (or decrease in the angle of
divergence) on upward gaze.
Considered significant if deviation differ by 10 Pd
7/15/2020Optom. Ankit varshney6
7.
2) V-pattern:-
“V”phenomenon in ESOphoria and
ESOtropia:- On looking directly
downwards the convergent
deviation is considerably greater
than when looking directly upwards.
“V” phenomenon in EXOphoria and
EXOtropia:- On looking directly
upwards the divergent deviation is
greater than when looking directly
downwards.
TYPES
ESO ↑ Downgaze
EXO ↑ Upgaze 7/15/2020Optom. Ankit varshney7
8.
“V” phenomenon
Theterm applied to those cases which show a
considerable increase in the angle of convergence (or
decrease in the angle of divergence) on downward
gaze.
Considered significant if deviation differ by 15 Pd
7/15/2020Optom. Ankit varshney8
9.
“X” pattern
“X”pattern or “X” exotropia:- The EXOdeviation more
in upward and downward gaze and less in the primary
position.
Patients with X pattern may fuse in primary position
but not necessarily
7/15/2020Optom. Ankit varshney9
10.
“Y” pattern
“Y”pattern or “Y” exotropia:- The EXOdeviation more
only in the upward gaze . Same and less in primary
position and downward gaze.
Patients with Y pattern may fuse in primary position but
not necessarily
7/15/2020Optom. Ankit varshney10
11.
“◊” pattern
“◊”pattern or “◊” exotropia {Diamond exotropia
:- The exodeviation is more in primary position.
Eyes are more closer or divergence less in the
upward and downward gazes.
7/15/2020Optom. Ankit varshney11
12.
“” pattern
“”pattern or “” exotropia:- The exodeviation is
more only in downward gaze. Same and less in
primary position and upward gaze.
Patients with pattern may fuse in primary
position but not necessarily
7/15/2020Optom. Ankit varshney12
13.
The physiological variation
This happens in the normal eyes in the absence
of any squint.
In this, there is a slight relative divergence in
supraversion and a slight relative convergence in
infraversion.
It is considered ‘physiological’ only if it is of
slight degree.
The difference in the angle of deviation on 7/15/2020Optom. Ankit varshney13
14.
While measuring theA-V pattern, certain
criteria's considered are:-
1) The deviation should be measured by means of the
prism and cover test with eyes in the mid-line position.
2) The patient should wear the full correction for his
error of refraction.
3) The fixation target should be small.
4) In making the measurements with the eyes looking
upwards and downwards, the extent of the eye
movements should be not more than 25° above and
below the mid-line respectively.
5) The measurements should be made with a fixation
object at a distance of 20 feet.
7/15/2020Optom. Ankit varshney14
15.
AETIOLOGY
The aetiologyof vertically incomitant horizontal strabismus has
been argued for years.
Synthesis of these theories concludes that the most likely
muscles involved are either the horizontal muscles or the
cyclovertical muscles (obliques/vertical rectii) or a combination
of both.
V pattern: Brown, IO overaction, SO underaction, SR
underaction, LR overaction, Craniofacial anomalies.
A pattern: SO overaction, IO underaction, LR & IR
underaction.
7/15/2020Optom. Ankit varshney15
16.
1. HORIZONTAL SCHOOL
This first theory was put forward by URIST.
He supported the role of horizontal recti,
assuming that lateral recti are more effective
in up-gaze and medial recti are more effective
in downgaze.
Based on this Urist advocates surgery to correct
the said anomaly ie. In case of overaction of the
rectii, recess(weak) them and in case of 7/15/2020Optom. Ankit varshney16
17.
1) R.E. L.E.
Anover action of lateral recti causes V-
exotropia.
(lateral recti are more effective in up-gaze)
It is caused by increase divergence in up gaze.
SR IO
MR
IR SO
SRIO
MR
IRSO
LRLR
EXO ↑ Upgaze
7/15/2020Optom. Ankit varshney17
18.
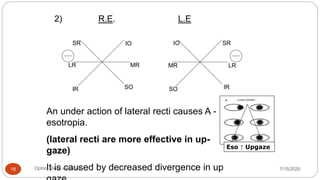
2) R.E. L.E
Anunder action of lateral recti causes A -
esotropia.
(lateral recti are more effective in up-
gaze)
It is caused by decreased divergence in up
SR SRIO IO
MRMR LR
IR IRSOSO
LR
Eso ↑ Upgaze
7/15/2020Optom. Ankit varshney18
19.
3) R.E. L.E.
Anover action of medial recti causes V-
esotropia
(medial recti are more effective in
downgaze.)
It is caused by increased convergence in
SR IO
MR
IR SO
SRIO
MR
IRSO
LRLR
ESO ↑ Downgaze
7/15/2020Optom. Ankit varshney19
20.
4) R.E. L.E.
Anunderaction of medial recti causes A -
exotropia.
(medial recti are more effective in
downgaze)
It is caused by decreased convergence in
downward gaze.
SR SRIO IO
MRMRLR LR
IR IRSOSO
Exo ↑ Downgaze
7/15/2020Optom. Ankit varshney20
21.
Pattern CAUSED BY
1.V-EXOtropia over action of LR
2. V-ESOtropia over action of MR
3. A-EXOtropia under action of MR
4. A-ESOtropia under action of LR
7/15/2020 Optom. Ankit varshney 21
22.
2. VERTICAL SCHOOL
Oblique overaction theory :-
Here the oblique's are thought to be involved.
Abduction is a tertiary action of the obliques. Their
overaction is commonly associated with either a
decrease in esodeviation or an increase in
exodeviation in upgaze or downgaze.
*Note:
With increasing abduction in upgaze, the inferior
obliques are thought to be overacting.
While increasing abduction in downgaze, the
superior obliques are thought to be overacting. 7/15/2020Optom. Ankit varshney22
23.
This secondtheory was put forward by BROWN.
He stressed the role of vertical recti in the etiology
of A-V patterns, the principle being the adducting
property of vertical recti.
However it seems logical to think that the actions of
vertical recti and oblique muscles are linked
inseparably.
7/15/2020Optom. Ankit varshney23
24.
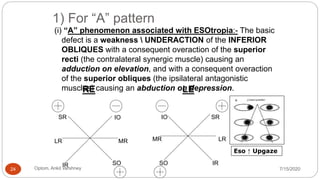
1) For “A”pattern
(i) “A” phenomenon associated with ESOtropia:- The basic
defect is a weakness UNDERACTION of the INFERIOR
OBLIQUES with a consequent overaction of the superior
recti (the contralateral synergic muscle) causing an
adduction on elevation, and with a consequent overaction
of the superior obliques (the ipsilateral antagonistic
muscles) causing an abduction on depression.
Eso ↑ Upgaze
LR LRMR MR
IO IO
SO SO
SR SR
IR IR
RE LE
7/15/2020Optom. Ankit varshney24
25.
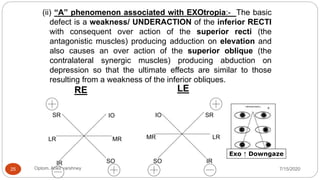
(ii) “A” phenomenonassociated with EXOtropia:- The basic
defect is a weakness/ UNDERACTION of the inferior RECTI
with consequent over action of the superior recti (the
antagonistic muscles) producing adduction on elevation and
also causes an over action of the superior oblique (the
contralateral synergic muscles) producing abduction on
depression so that the ultimate effects are similar to those
resulting from a weakness of the inferior obliques.
LR LRMR MR
IO IO
SO SO
SR SR
IR IR
RE LE
Exo ↑ Downgaze
7/15/2020Optom. Ankit varshney25
26.
2) For “V”pattern
(i) “V” phenomenon associated with ESOtropia:-
The basic defect is the weakness / UNDERACTION of the
SUPERIOR OBLIQUES with a consequent over action of the
inferior recti (the contra lateral synergist muscles) causing an
adduction on depression, and with a consequent over action
of inferior oblique (the ipsilateral antagonistic muscles)
causing an abduction of the eyes on elevation.
LR LRMR MR
IO IO
SO SO
SR SR
IR IR
RE LE
ESO ↑ Downgaze
7/15/2020Optom. Ankit varshney26
27.
(ii) “V” phenomenonassociated with Exotropia:- The
basic defect is weakness/ UNDERACTION of the
SUPERIOR RECTI which causes an over action of the
inferior recti (the ipsilateral antagonistic muscles) which is
responsible for the adduction on depression, and it also
causes an over action of the inferior obliques (the
contralateral synergic muscles) which is responsible for
abduction of the eyes on elevation.
LR LRMR MR
IO IO
SO SO
SR SR
IR IR
RE LE
EXO ↑ Upgaze
7/15/2020Optom. Ankit varshney27
28.
PATTERN and OVERACTINGMUSCLES
Overacting
muscle
Underacting
muscle
Pattern
caused
IO
IR
SO
SR
V pattern
SO
SR
IO
IR
A pattern
7/15/2020Optom. Ankit varshney28
29.
3) The thirdtheory
It says that they are the result of a combined
abnormality of action of the horizontally and
vertically acting muscles.
7/15/2020Optom. Ankit varshney29
30.
Aim
• To detectand measure the pattern
• To determine the reason for pattern if possible
• To asses it significant in the management of strabismus
7/15/2020Optom. Ankit varshney30
31.
Prerequisites;
1. Techniqueused to measure the deviation in up
gaze and down gaze.
Perfectly this should be done at distance
because at near an over convergence may
be produced in down gaze.
The accommodation should always be
controlled for both distance and near
measurement. Hence the full refractive
correction should be worn.
Otherwise, problems as accommodation and
over convergence at near will produce
spuriously high incidence of V-patterns.
7/15/2020Optom. Ankit varshney31
32.
AHP
May adopt toget gid of symptom.
*V eso and A exo chin
depressed .
* V exo and A eso chin elevated
.
7/15/2020Optom. Ankit varshney32
33.
• Cover test
•Ocular movement
• Measurement of deviation with
PCT
• Investigation of binocular
function
• Hess chart .
7/15/2020Optom. Ankit varshney33
34.
Evaluation:
Measurement - Adults
PBCT* acco.target - 6mts / 33cms
* primary,25˙up & 25˙ down
* moving target /chin up-down
• For A-pattern, there should be at least 10 of
greater esodeviation (or lesser exodeviation)
in up gaze as compared with down gaze.
• For diagnosis of a V-pattern at least 15
greater exodeviation (or lesser esodeviation)
is required in up gaze than in down gaze. 7/15/2020Optom. Ankit varshney34
35.
Evaluation:
Measurement - Children
Krimsky’s/Hirschberg’s
Problems;
* lack of cooperation
* short attention span
* incomplete development of following
movement.
7/15/2020Optom. Ankit varshney35
36.
Evaluation:
A: Motor *Bino/Uniocular move.9 gazes
* Oblique dysfunction
* Torsion- maddox double rod
B: Sensory * Bagolini’s
- preferred posture
- all 3 vertical gazes
7/15/2020Optom. Ankit varshney36
2) Symptoms andsigns
Patients with A-V patterns are frequently
troubled with intermittent transient diplopia.
For this reason, they may assume various head
postures.
Cosmetic problem.
If the patient has fusion potential, aesthenopia
can be so common symptom.
7/15/2020Optom. Ankit varshney41
42.
MANAGEMENT
The managementdepends on the clinical factors. If
the pattern is significant and symptomatic,
SURGERY is needed.
All cases of esodeviation or exodeviation should
be checked for A or V pattern. In case of oblique
over action being present, the obliques should be
weakened. In case of under action, the same should
be strengthened.
7/15/2020Optom. Ankit varshney42
43.
TREATMENT
Thecurrent therapy of vertically incomitant
horizontal strabismus is surgical.
Recession:- It is the procedure in which rectus or
oblique muscle is disinserted /removed from its
original position and is reinserted slightly posterior
to the original insertion position.
7/15/2020Optom. Ankit varshney43
44.
Three surgicalprinciples are involved.
These are :-
i. Weakens overacting obliques if either the superior or
inferior obliques are overacting.
ii. If both the superior and inferior obliques are
overacting, weakening of any oblique muscle is
contraindicated.
iii. Vertically transpose the horizontal recti if the oblique
are not overacting.
7/15/2020Optom. Ankit varshney44
ROLE OF AN
OPTOMETRIST
Pre-operative examination.
Post-operative checkup.
Help and maintain to keep B.S.V. if there is B.S.V.
7/15/2020Optom. Ankit varshney47