- Coronary CT angiography uses x-rays and contrast material to examine the coronary arteries with high spatial and temporal resolution. It is non-invasive compared to traditional coronary angiography.
- Key factors for cardiac imaging include high temporal resolution (<250ms), spatial resolution (<0.75mm), and synchronization with the cardiac cycle using ECG gating. Prospective and retrospective gating, partial and multi-segment reconstruction, and low pitch values (<0.5) help achieve this.
- Advances in multi-detector CT scanners, faster gantry rotation times (<330ms), and improved reconstruction algorithms now allow temporal resolutions as low as 80ms for coronary CT angiography.








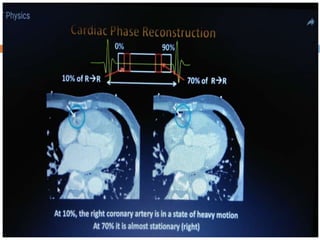





















![Misalignment and Slab Artifacts:
Occur especially in patients with high heart
rates, heart rate variability, and the presence
of irregular or ectopic heart beats (e.g.,
premature ventricular contractions [PVCs] and
atrial fibrillation)
can be best recognized in a sagittal or coronal
view.
Often limit the diagnostic assessment of
coronary artery segments.
One option is to reconstruct the dataset at
different phases of the cardiac cycle.](https://image.slidesharecdn.com/coronaryctangiogram-200128052745/85/Coronary-CT-angiogram-physics-42-320.jpg)