Downloaded 226 times

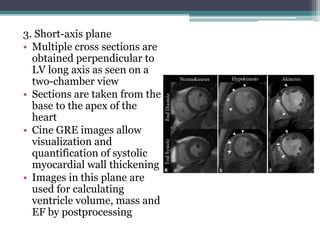
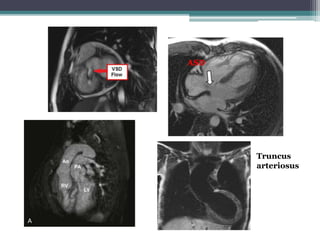
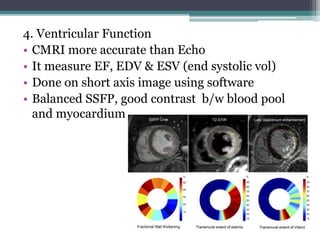
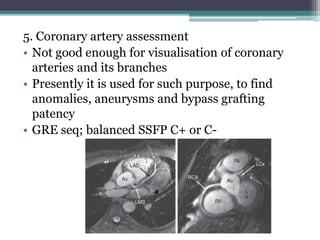

This document discusses cardiac MRI (CMRI) and its clinical applications. CMRI provides anatomical and functional information to assess heart abnormalities through various sequences like ECG-gated bright and dark blood sequences. It is useful for evaluating congenital heart diseases, valvular heart diseases, ventricular function, coronary arteries, myocardial perfusion and viability, cardiac masses, and pericardial diseases. CMRI is more accurate than echocardiography for measuring ejection fraction, volumes, and assessing ventricular function and viability. It is useful for differentiating conditions like arrhythmogenic right ventricular dysplasia, restrictive vs constrictive cardiomyopathy, and determining feasibility of revascularization procedures.















































































