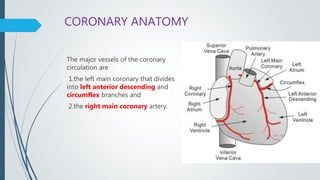
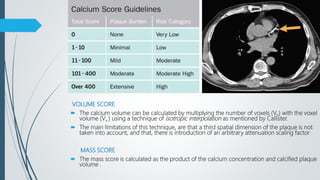
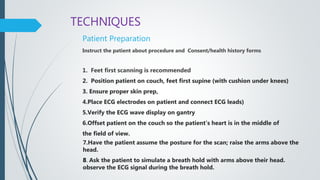
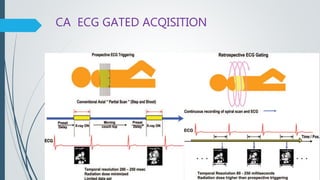
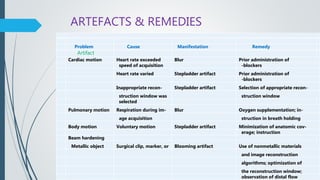
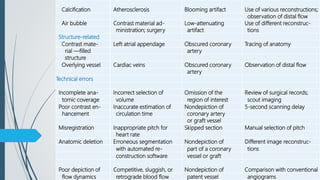
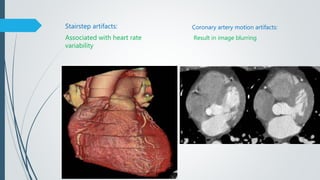
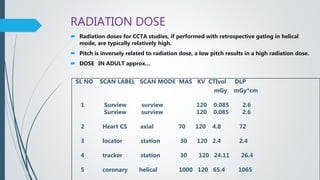
The document provides an overview of coronary CT angiography (CCTA). It discusses recent advances in CCTA technology including perfusion imaging, spectral imaging, and fractional flow reserve CT (FFR-CT). The anatomy and physiology of the coronary arteries is described. The document outlines the equipment, indications, procedures, and post-processing techniques used in CCTA. It also discusses calcium scoring, artifacts, case studies, radiation dose, and limitations of CCTA.