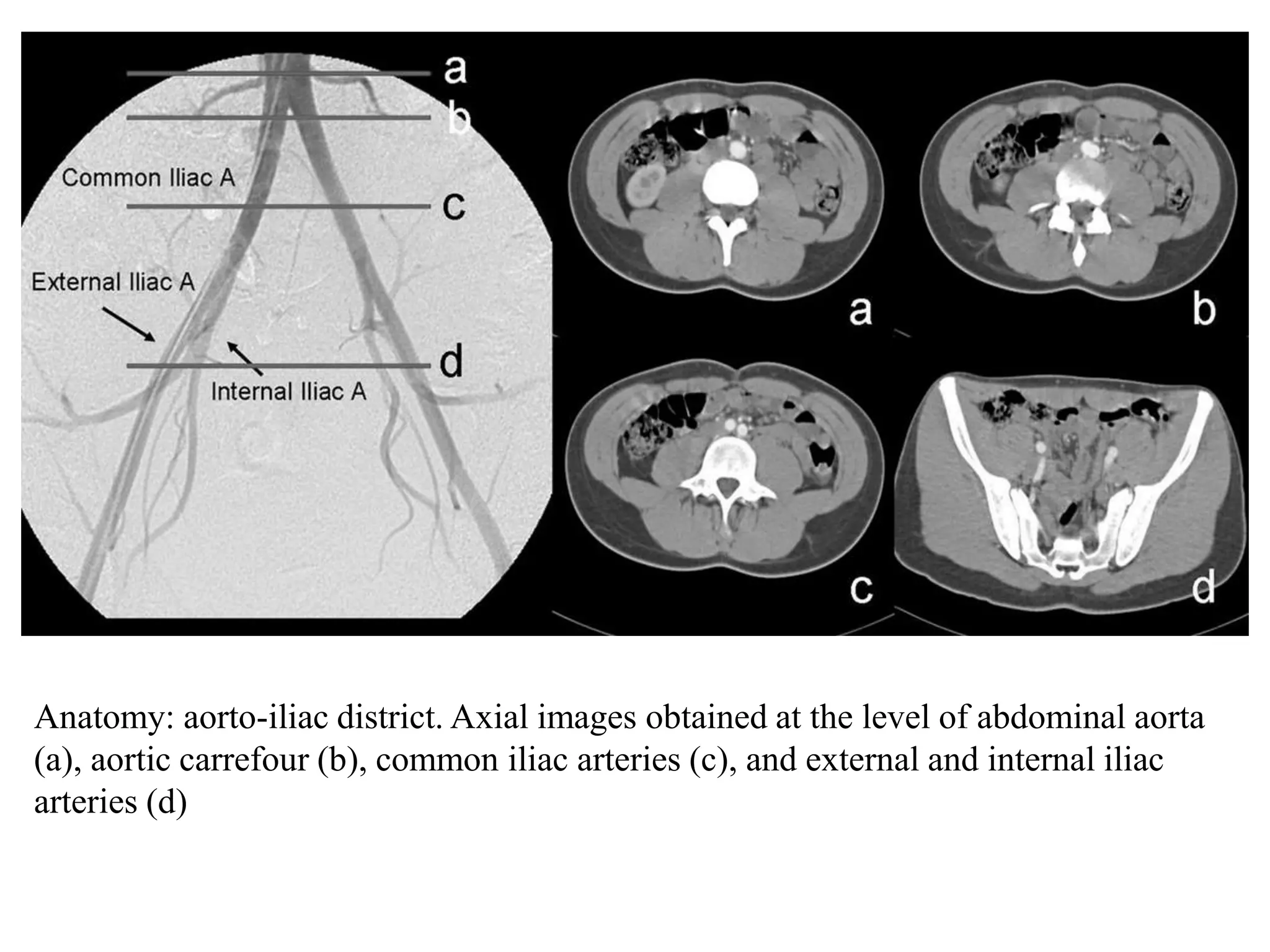
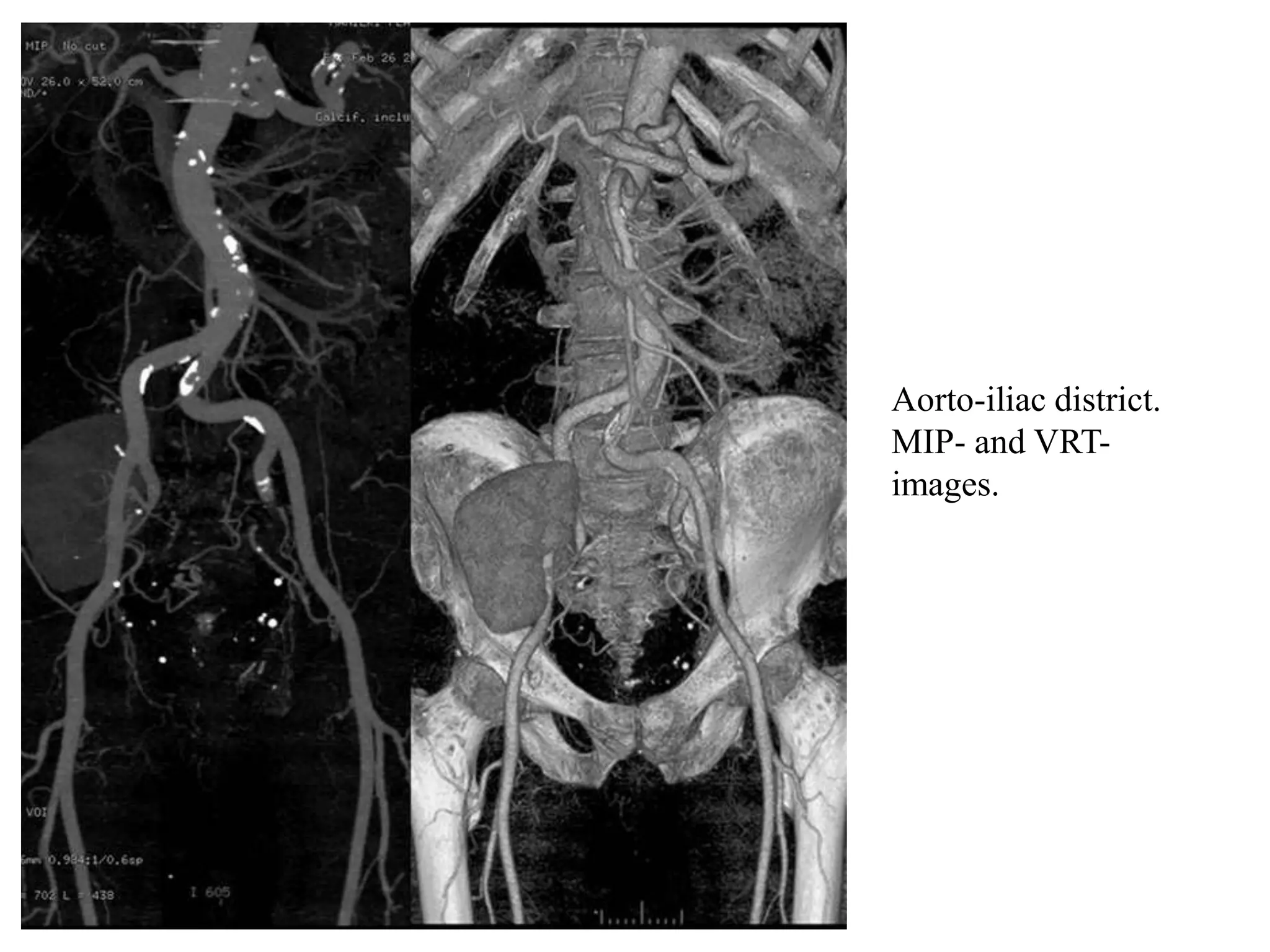
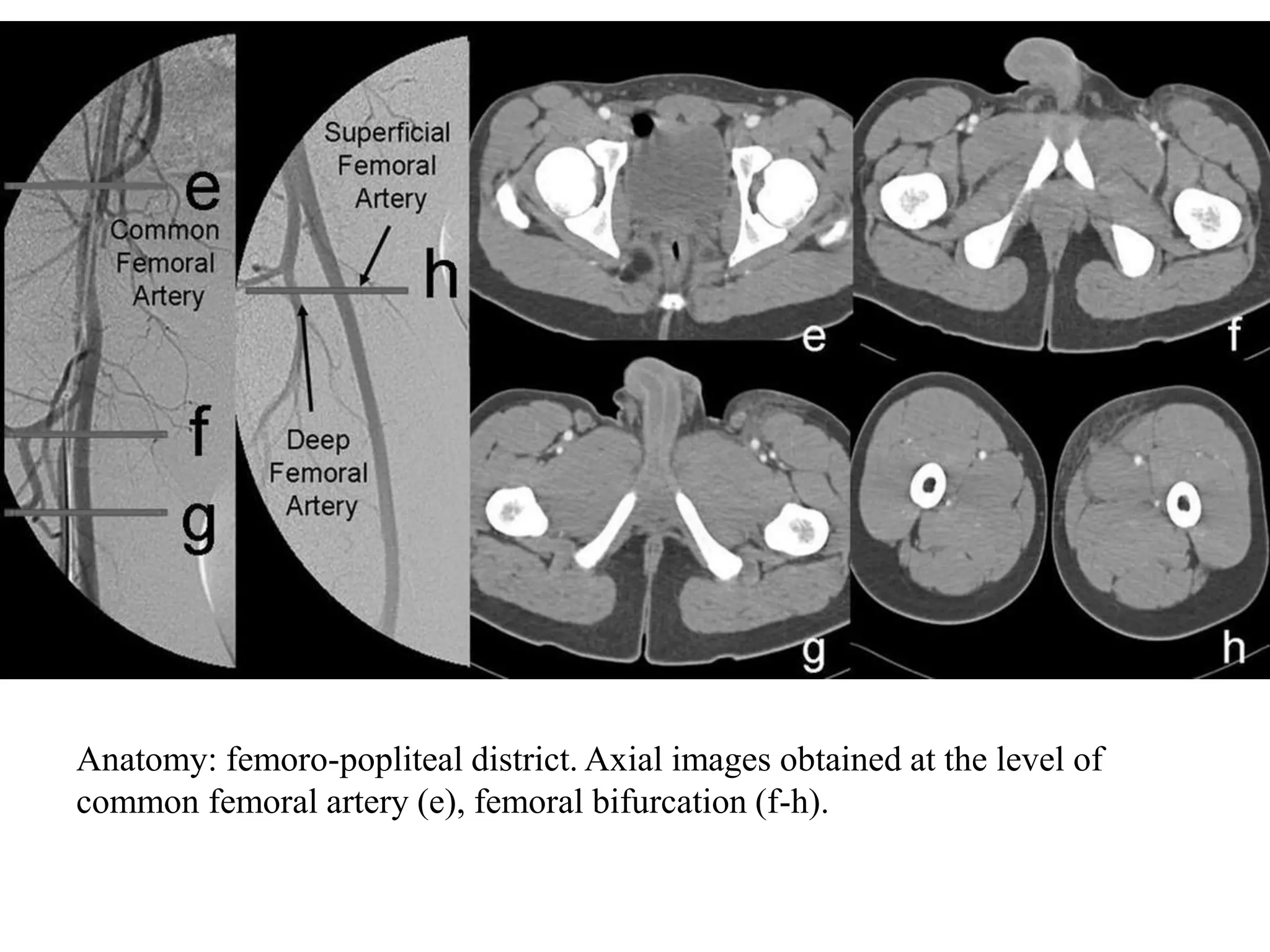
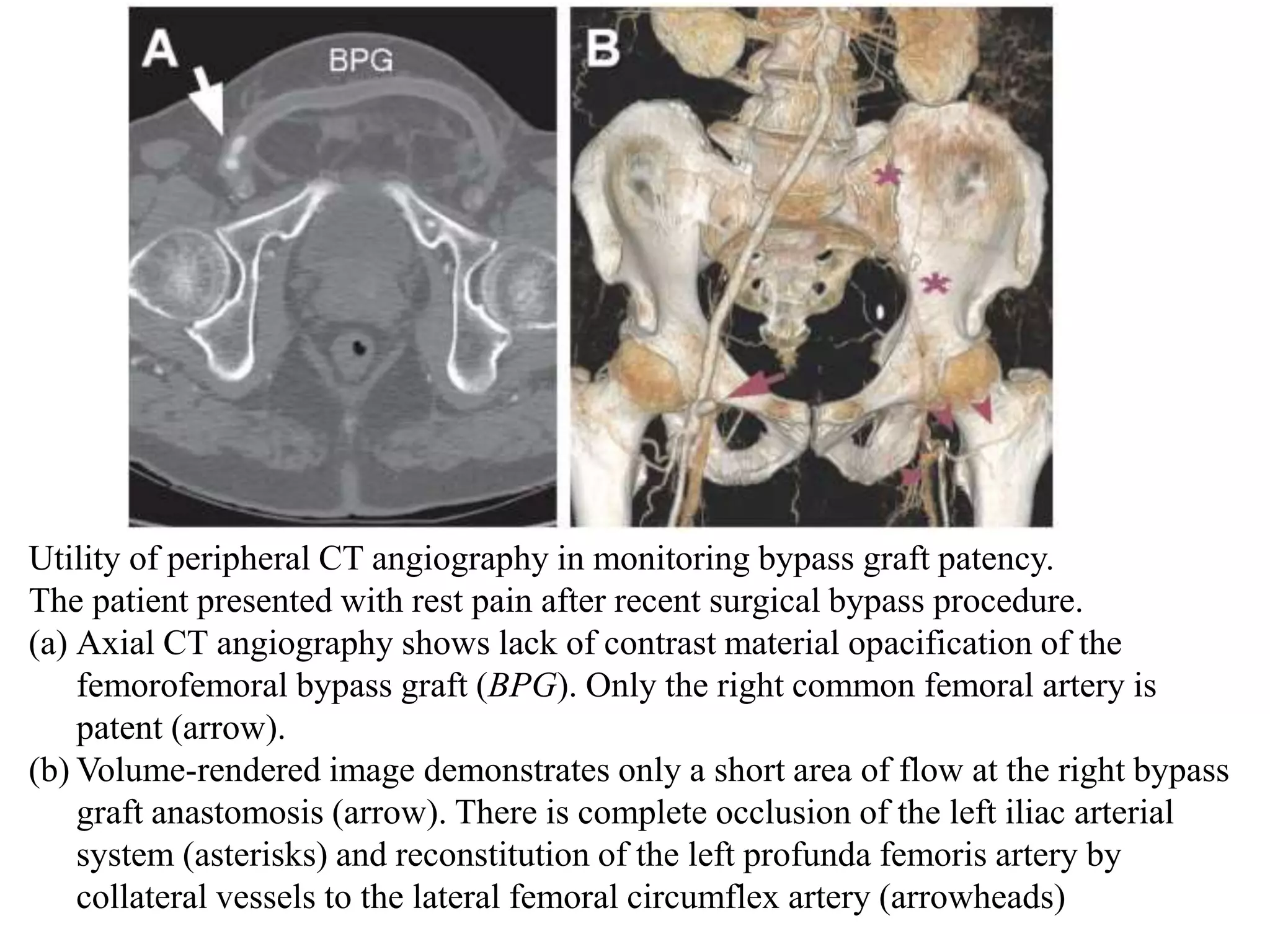
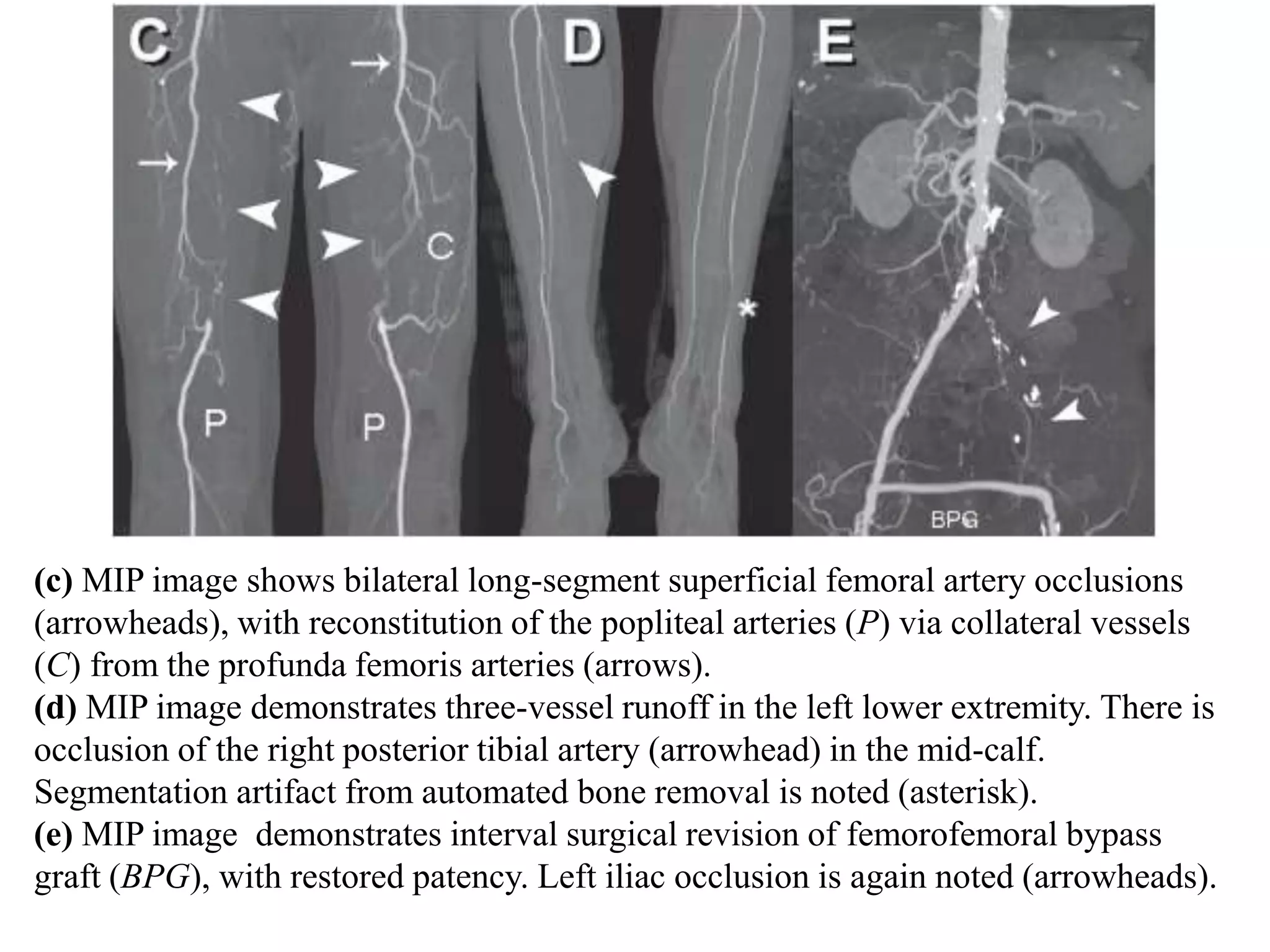
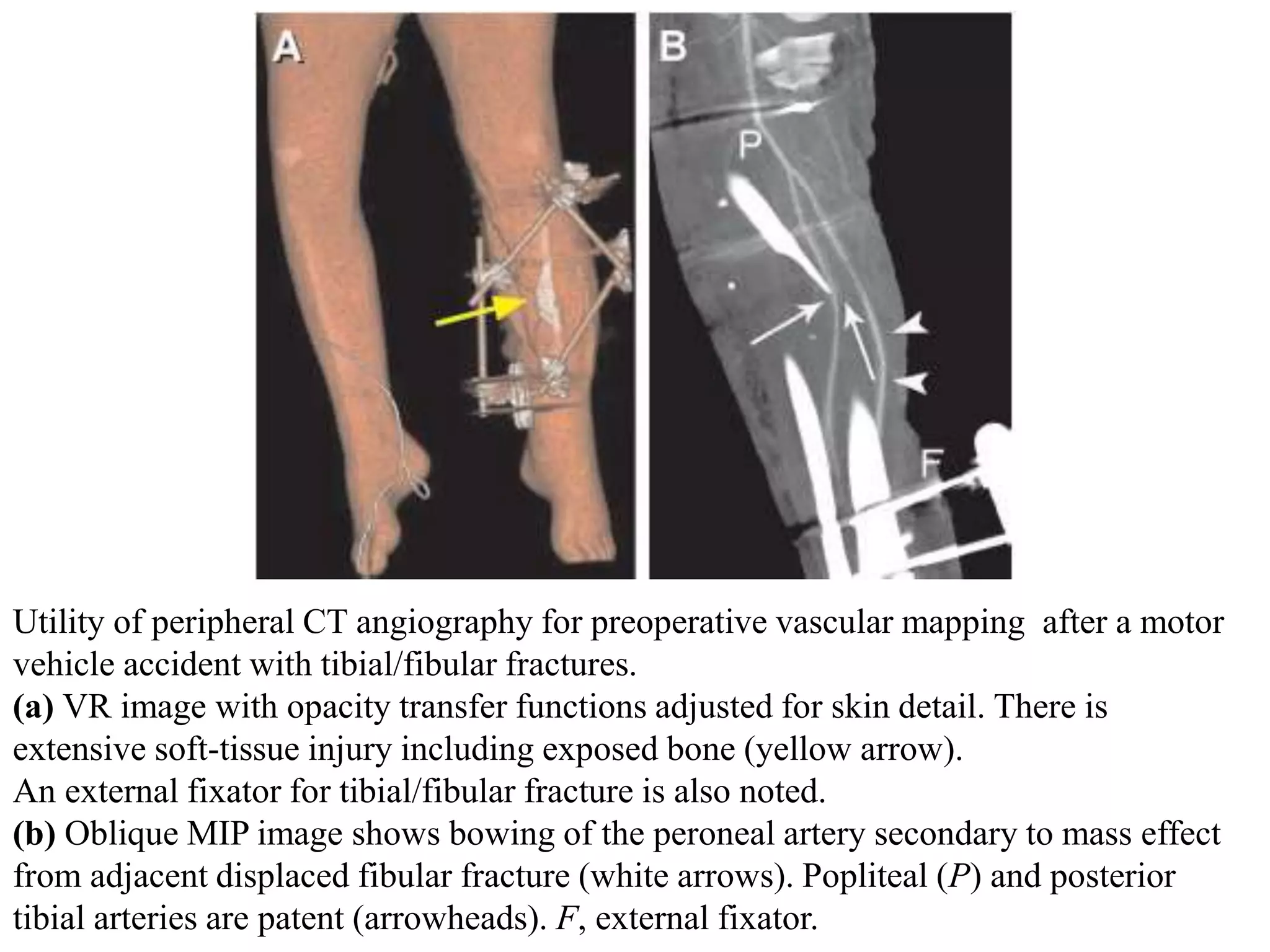
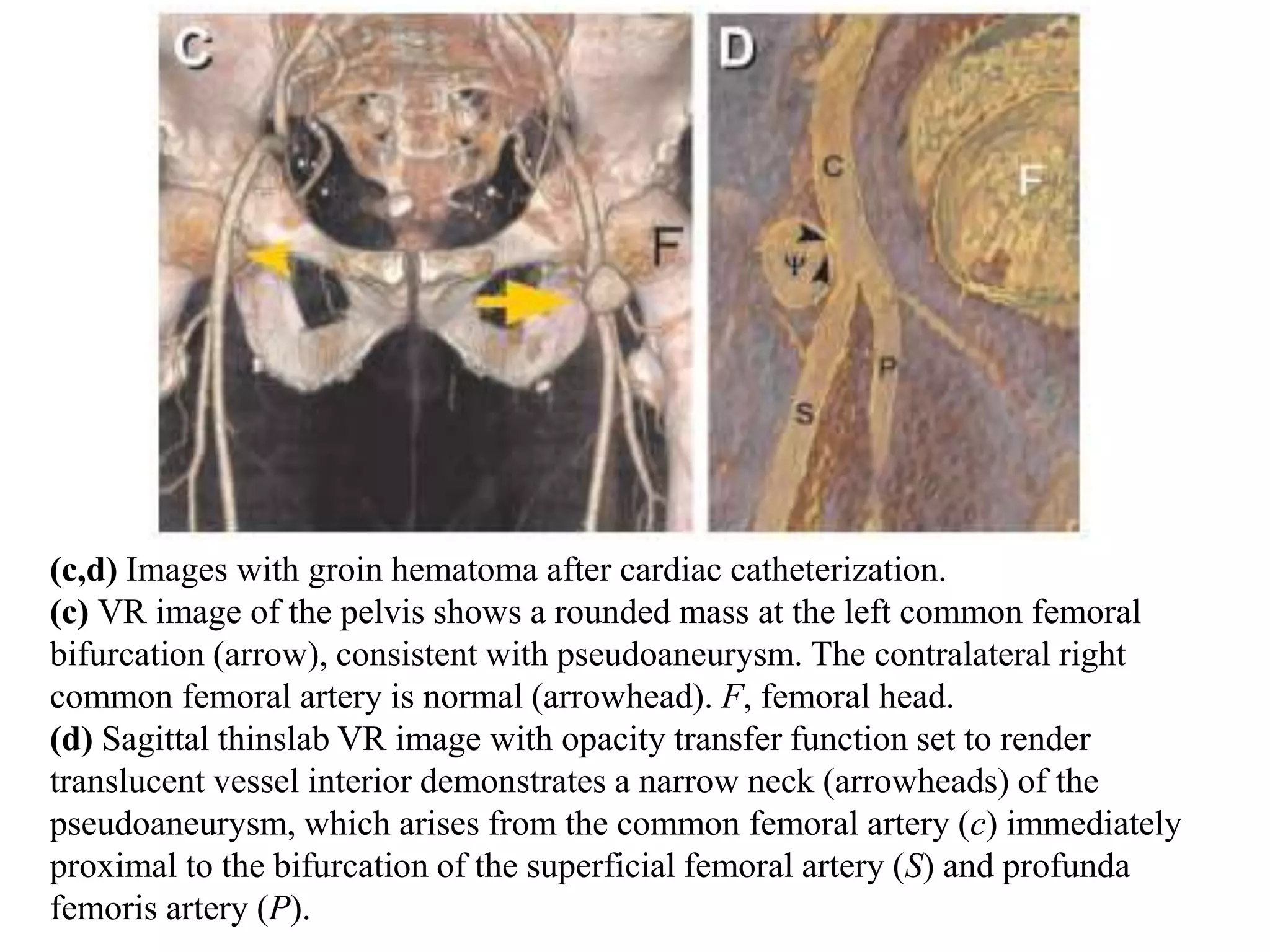
This document provides information on performing and interpreting CT angiography of the lower limbs. It discusses scanning techniques, protocols, contrast injection, and principles of timing acquisitions. Image post-processing includes MIP, VR, and MPR. Interpretation requires scrutinizing calcifications and stents to avoid overestimating stenosis. Peripheral CTA is useful for evaluating occlusive disease, aneurysms, trauma, infections, embolism, and postoperative surveillance. Examples demonstrate various vascular pathologies.














































































![Peripheral_Vascular_Injuries_Presentation[1][1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/peripheralvascularinjuriespresentation11-250707170227-54480eba-thumbnail.jpg?width=640&height=640&fit=bounds)










































