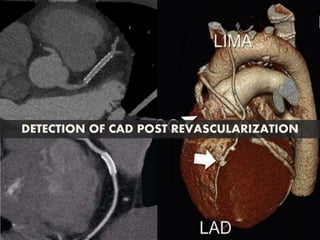
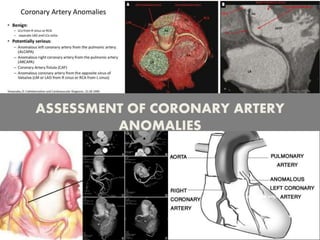
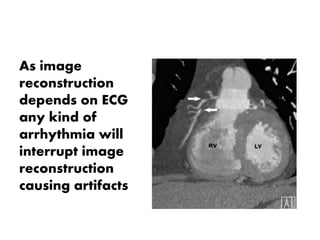
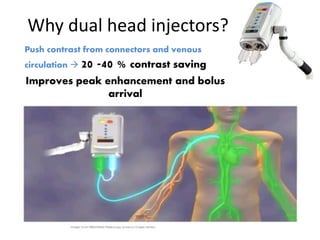
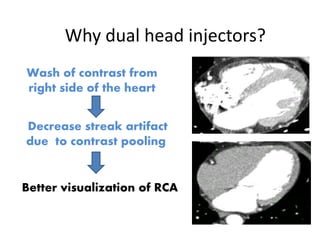
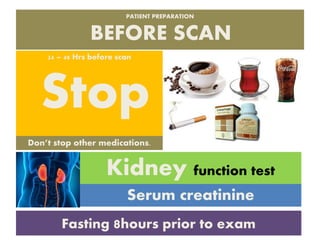
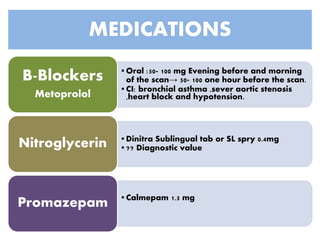
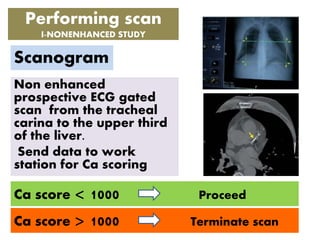
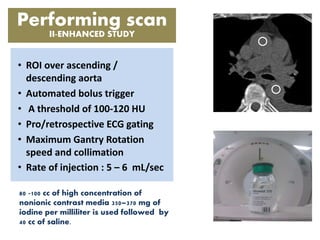
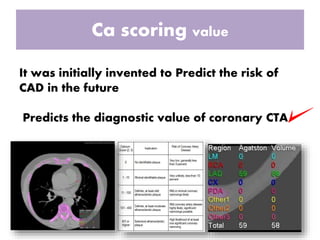
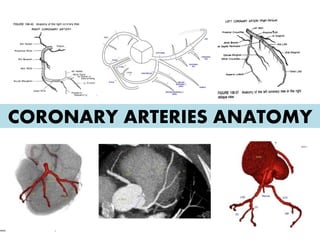
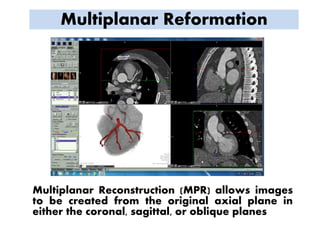
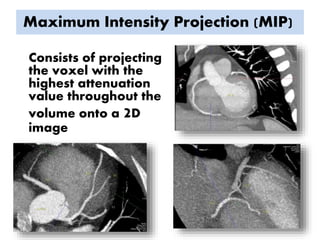
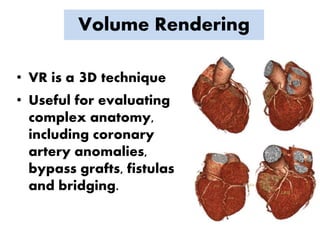
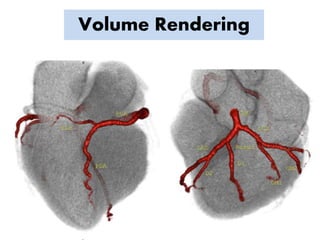
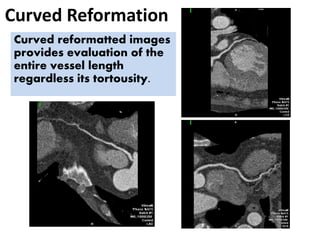
Coronary CT angiography allows for noninvasive imaging of the heart and coronary arteries. It can be used to evaluate patients with chest pain, assess coronary arteries after revascularization, and detect congenital coronary anomalies. The scan involves a non-contrast scan for calcium scoring followed by a contrast-enhanced scan. Proper patient preparation including beta-blockers and nitroglycerin is important. Images are analyzed using techniques like multiplanar reformation, maximum intensity projection, volume rendering and curved reformation to evaluate coronary artery anatomy and detect any stenosis.