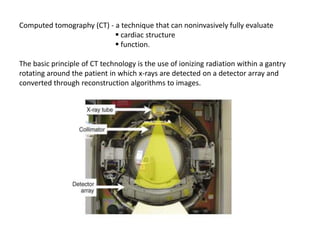
CT provides noninvasive evaluation of cardiac structure and function. It uses ionizing radiation and reconstruction algorithms to form images. Advancements include increasing detector rows for wider coverage and shorter scan times. CT can assess coronary calcium scoring, coronary angiography, bypass graft/stent patency, cardiac morphology/function, and pericardial diseases. It is useful for diagnosing chest pain, coronary anomalies, and evaluating surgical candidates. Risks include radiation exposure and contrast nephropathy, so appropriate patient selection is important.