![s
*****of apprehension[…fear..] e.g. by opioid
like drugs as meperidine I.M. 25 mg.
s Subsequent dental ttt…
s Episodes of H.F. should be considered.](https://image.slidesharecdn.com/congestiveheartfailure-140122215310-phpapp01/85/Congestive-heart-failure-28-320.jpg)

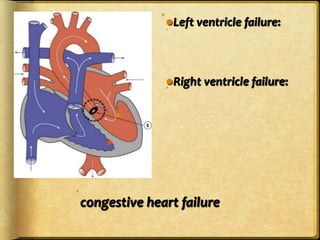
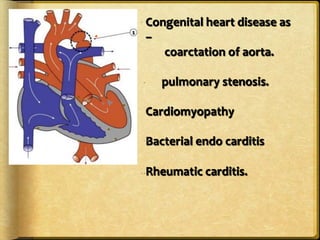
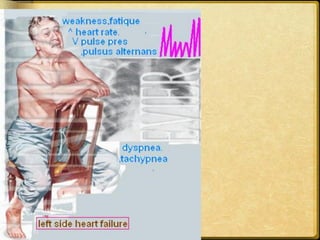
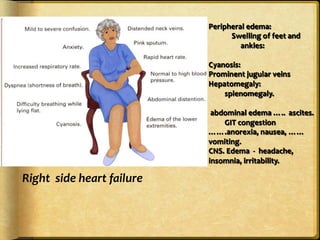
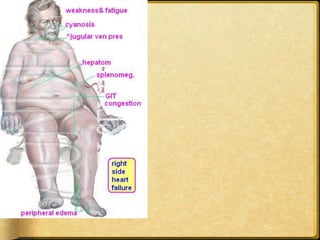
This document discusses heart failure, including its definitions, types, causes, clinical manifestations, and management from a dental perspective. It defines heart failure as the heart's inability to supply sufficient oxygenated blood to the body's needs. The types include left ventricle, right ventricle, and combined failure. Causes include congenital heart defects and conditions like cardiomyopathy. Clinical manifestations vary depending on which ventricle is affected but may include edema, dyspnea, fatigue, and cyanosis. Dental management involves recognizing signs of failure, terminating procedures if needed, positioning the patient comfortably, and providing post-procedure care and follow-up.































































































