Congestive Heart Failure(CHF)
Congestive heart failure (CHF) is defined as a chronic
progressive condition where the heart is unable to
pump enough blood to meet the body's needs,
resulting in fluid buildup in the lungs, liver, and
peripheral tissues.
3.
Definition of CongestiveHeart Failure (CHF)
The American Heart Association (AHA) defines congestive heart
failure (CHF) as a chronic progressive condition where the
heart's output is insufficient to meet the body's needs, resulting
in fluid buildup in the lungs, liver, and peripheral tissues. This
condition occurs when the heart fails to pump enough blood,
leading to congestion in the lungs and other parts of the body.
4.
Etiology
H -HTN
E – Endocarditis
A – Anemia
R - RHD
T – Thyrotoxicosis
F – Failure to take medicine
A – Arrythmia
I – Infection & ischemia
L – Lungs problem (COPD &
PE)
E – Endocrine
D – Dietary Indiscretions
5.
Types of HeartFailure
Type Key Problem Main Symptoms
Left-sided
HF
Pulmonary
congestion
Dyspnoea, crackles, orthopnoea, PND
Right-sided
HF
Systemic congestion Peripheral edema, JVD, ascites
Systolic HF
Pumping/
contractility
problem
↓ Ejection Fraction (<40%), fatigue,
pulmonary edema
6.
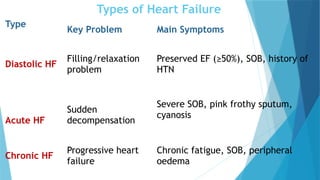
Types of HeartFailure
Type
Key Problem Main Symptoms
Diastolic HF
Filling/relaxation
problem
Preserved EF (≥50%), SOB, history of
HTN
Acute HF
Sudden
decompensation
Severe SOB, pink frothy sputum,
cyanosis
Chronic HF
Progressive heart
failure
Chronic fatigue, SOB, peripheral
oedema
7.
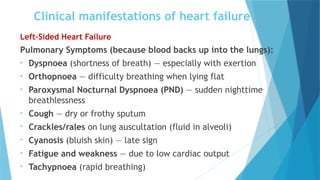
Clinical manifestations ofheart failure
Left-Sided Heart Failure
Pulmonary Symptoms (because blood backs up into the lungs):
• Dyspnoea (shortness of breath) — especially with exertion
• Orthopnoea — difficulty breathing when lying flat
• Paroxysmal Nocturnal Dyspnoea (PND) — sudden nighttime
breathlessness
• Cough — dry or frothy sputum
• Crackles/rales on lung auscultation (fluid in alveoli)
• Cyanosis (bluish skin) — late sign
• Fatigue and weakness — due to low cardiac output
• Tachypnoea (rapid breathing)
8.
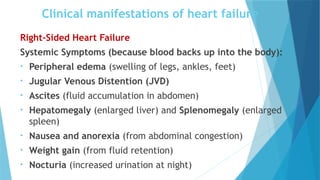
Clinical manifestations ofheart failure
Right-Sided Heart Failure
Systemic Symptoms (because blood backs up into the body):
• Peripheral edema (swelling of legs, ankles, feet)
• Jugular Venous Distention (JVD)
• Ascites (fluid accumulation in abdomen)
• Hepatomegaly (enlarged liver) and Splenomegaly (enlarged
spleen)
• Nausea and anorexia (from abdominal congestion)
• Weight gain (from fluid retention)
• Nocturia (increased urination at night)
9.
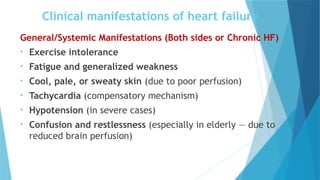
Clinical manifestations ofheart failure
General/Systemic Manifestations (Both sides or Chronic HF)
• Exercise intolerance
• Fatigue and generalized weakness
• Cool, pale, or sweaty skin (due to poor perfusion)
• Tachycardia (compensatory mechanism)
• Hypotension (in severe cases)
• Confusion and restlessness (especially in elderly — due to
reduced brain perfusion)
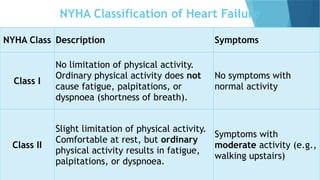
NYHA Classification ofHeart Failure
NYHA Class Description Symptoms
Class I
No limitation of physical activity.
Ordinary physical activity does not
cause fatigue, palpitations, or
dyspnoea (shortness of breath).
No symptoms with
normal activity
Class II
Slight limitation of physical activity.
Comfortable at rest, but ordinary
physical activity results in fatigue,
palpitations, or dyspnoea.
Symptoms with
moderate activity (e.g.,
walking upstairs)
12.
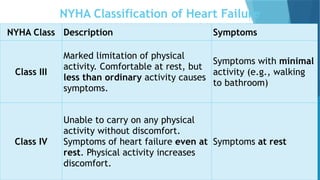
NYHA Classification ofHeart Failure
NYHA Class Description Symptoms
Class III
Marked limitation of physical
activity. Comfortable at rest, but
less than ordinary activity causes
symptoms.
Symptoms with minimal
activity (e.g., walking
to bathroom)
Class IV
Unable to carry on any physical
activity without discomfort.
Symptoms of heart failure even at
rest. Physical activity increases
discomfort.
Symptoms at rest
13.
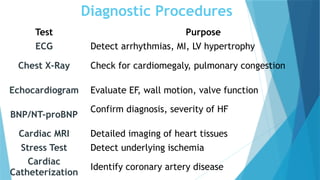
Diagnostic Procedures
Test Purpose
ECGDetect arrhythmias, MI, LV hypertrophy
Chest X-Ray Check for cardiomegaly, pulmonary congestion
Echocardiogram Evaluate EF, wall motion, valve function
BNP/NT-proBNP
Confirm diagnosis, severity of HF
Cardiac MRI Detailed imaging of heart tissues
Stress Test Detect underlying ischemia
Cardiac
Catheterization
Identify coronary artery disease
14.
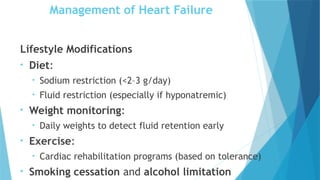
Management of HeartFailure
Lifestyle Modifications
• Diet:
• Sodium restriction (<2–3 g/day)
• Fluid restriction (especially if hyponatremic)
• Weight monitoring:
• Daily weights to detect fluid retention early
• Exercise:
• Cardiac rehabilitation programs (based on tolerance)
• Smoking cessation and alcohol limitation
15.
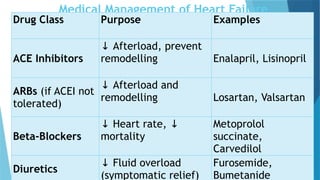
Medical Management ofHeart Failure
Drug Class Purpose Examples
ACE Inhibitors
↓ Afterload, prevent
remodelling Enalapril, Lisinopril
ARBs (if ACEI not
tolerated)
↓ Afterload and
remodelling Losartan, Valsartan
Beta-Blockers
↓ Heart rate, ↓
mortality
Metoprolol
succinate,
Carvedilol
Diuretics
↓ Fluid overload
(symptomatic relief)
Furosemide,
Bumetanide
16.
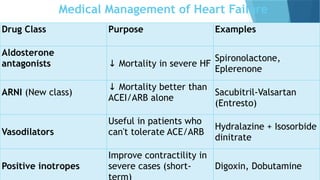
Medical Management ofHeart Failure
Drug Class Purpose Examples
Aldosterone
antagonists ↓ Mortality in severe HF
Spironolactone,
Eplerenone
ARNI (New class)
↓ Mortality better than
ACEI/ARB alone
Sacubitril-Valsartan
(Entresto)
Vasodilators
Useful in patients who
can't tolerate ACE/ARB
Hydralazine + Isosorbide
dinitrate
Positive inotropes
Improve contractility in
severe cases (short- Digoxin, Dobutamine
17.
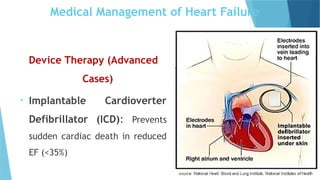
Device Therapy (Advanced
Cases)
•Implantable Cardioverter
Defibrillator (ICD): Prevents
sudden cardiac death in reduced
EF (<35%)
Medical Management of Heart Failure
18.
Cardiac Resynchronization Therapy(CRT):
CRT is a specialized treatment for heart failure where a
biventricular pacemaker is implanted to help the right and
left ventricles contract together (synchronously).
This improves heart efficiency, reduces symptoms, and
increases survival.
Medical Management of Heart Failure
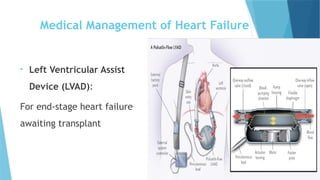
19.
• Left VentricularAssist
Device (LVAD):
For end-stage heart failure
awaiting transplant
Medical Management of Heart Failure
20.
Surgical Management
• HeartTransplant:
For patients with refractory (end-stage) heart failure.
• Coronary Artery Bypass Grafting (CABG):
If HF is due to significant coronary artery disease.
Nursing Management ofHeart Failure
Improve Oxygenation
• Position in high-Fowler’s if dyspneic.
• Administer supplemental oxygen as ordered.
• Monitor ABGs if needed.
24.
Nursing Management ofHeart Failure
Manage Fluid Overload
• Administer diuretics (e.g., furosemide) as prescribed.
• Restrict fluids and sodium* if ordered.
• Track daily weight — report gain >2-3 lbs in a day.
25.
Nursing Management ofHeart Failure
Enhance Cardiac Function
• Administer cardiac medications: ACE inhibitors, beta-blockers,
digoxin, etc as per prescription.
• Monitor for medication side effects (e.g., hypotension,
bradycardia, digoxin toxicity).
26.
Nursing Management ofHeart Failure
Plan rest periods between activities.
Provide Education
• Teach about low-sodium diet.
• Instruct on medication adherence.
• Teach signs of worsening CHF: weight gain, swelling, increased
SOB.
• Emphasize the importance of follow-up appointments.