Downloaded 3,565 times


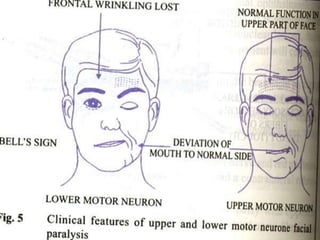
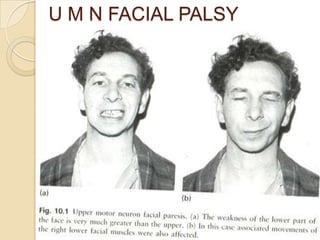
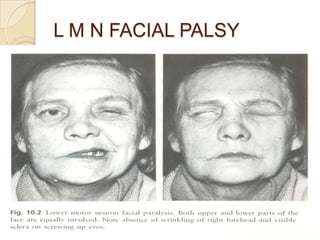
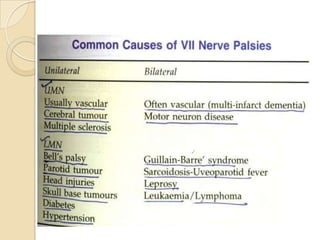
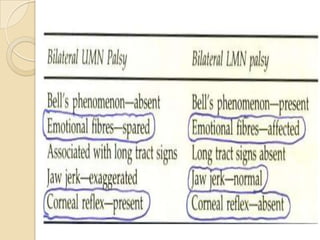
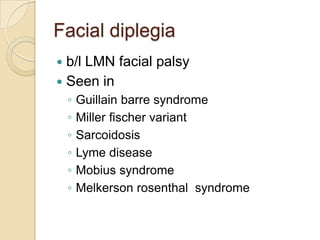
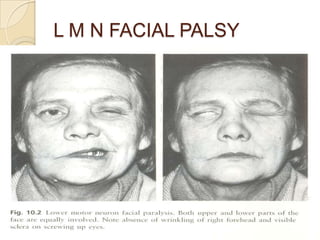
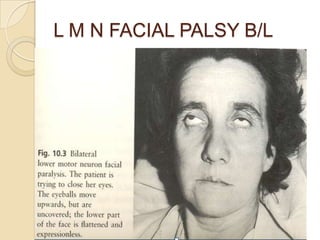


The document discusses facial palsy, particularly Bell's palsy, which is an acute, idiopathic lower motor neuron facial paralysis. It outlines the clinical presentation, diagnosis, and treatment options, emphasizing the importance of early intervention for better prognosis. Approximately 80% of patients recover within a few weeks, with various factors influencing recovery outcomes, including the severity of the palsy at presentation.























































































