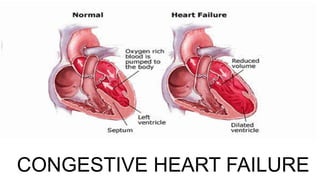
The seminar outlines the understanding of cardiovascular emergencies, specifically highlighting conditions like congestive heart failure (CHF), myocardial infarction (MI), and acute pulmonary issues. It covers the definitions, clinical manifestations, diagnostic assessments, and management strategies for these conditions, as well as nursing interventions and the epidemiology of heart failure. The document emphasizes the importance of rapid recognition and treatment to reduce morbidity and mortality in affected patients.








![1.Decrease activity of coagulation system with
pharmacologic therapy:
Antiplatelet agents: aspirin, GP IIb/IIIa receptor blocking agents (e.g.,
abciximab [Reopro], eptitbatide [Integrilin], and tirofiban [Aggrastat]),
thienopyridine agents (e.g., clopidogrel [Plavix])
Antithrombin agents: Indirect (e.g., heparin, low molecular-weight
heparin), direct (e.g., bivalirudin)
MANAGEMENT OF MI(MEDICAL)](https://image.slidesharecdn.com/cardioemergenciesi-230119185732-3f8ef1bc/85/cardio-emergencies-I-pptx-55-320.jpg)












![NURSING DIAGNOSIS
Risk for bleeding related to anticoagulant or thrombolytic therapy.
• Assess for the signs and symptoms of bleeding from catheter insertion sites, bleeding
from mucous membranes, decreased haematocrit and haemoglobin, gastrointestinal
bleeding, genitourinary bleeding, hematoma, petechiae, purpura, respiratory tract
bleeding.
• Monitor platelet counts, coagulation test results (INR), PT, activated partial thromboplastin
time [aPTT], and haemoglobin and haematocrit. Notify the physician immediately if a
higher or lower than the designated range occurs.
• If the client is HIPA positive, stop all heparin products and consult a haematologist.](https://image.slidesharecdn.com/cardioemergenciesi-230119185732-3f8ef1bc/85/cardio-emergencies-I-pptx-101-320.jpg)
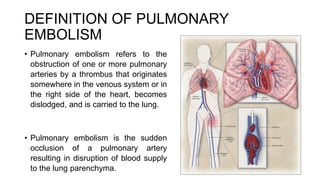
![DEFINITION OF CARDIOGENIC
SHOCK
• Shock is the inability of the circulatory system to deliver enough
blood to meet the oxygen and nutrient requirements of body
tissues.
• Cardiogenic shock (CS) is characterized by systemic
hypoperfusion due to severe depression of the cardiac index
[18 mmHg].
• It is associated with in-hospital mortality rates >50%.](https://image.slidesharecdn.com/cardioemergenciesi-230119185732-3f8ef1bc/85/cardio-emergencies-I-pptx-103-320.jpg)



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)








