

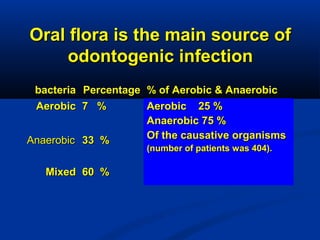
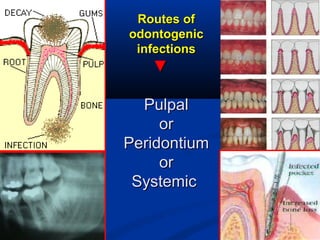

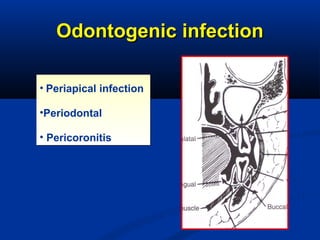
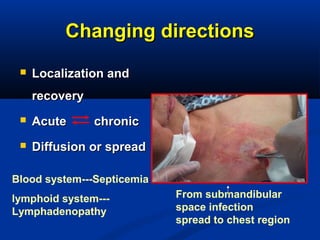
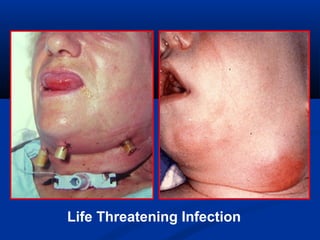



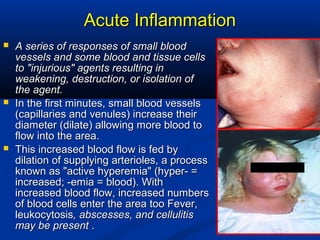



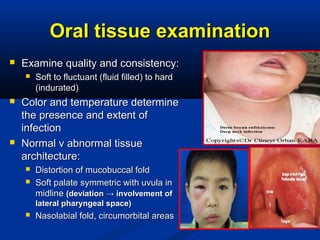
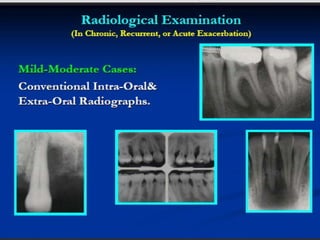
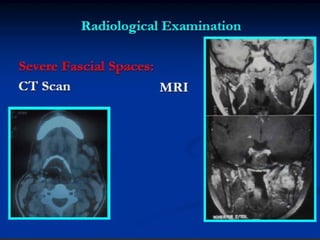
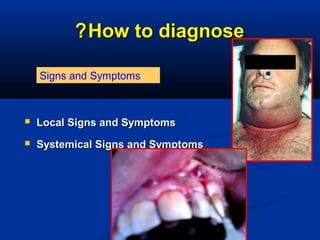
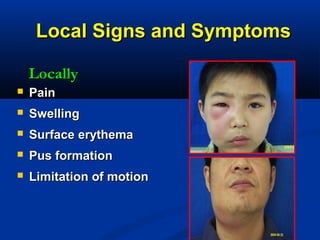
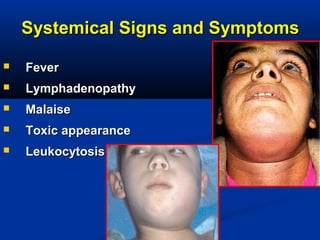
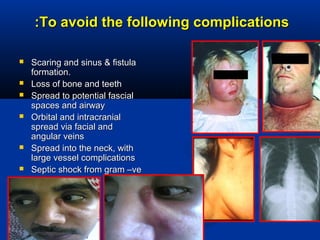

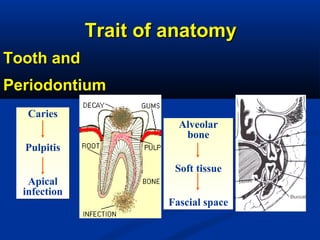
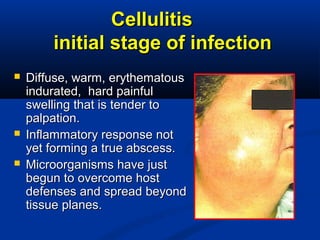
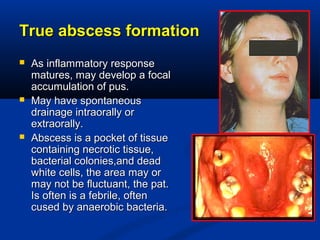
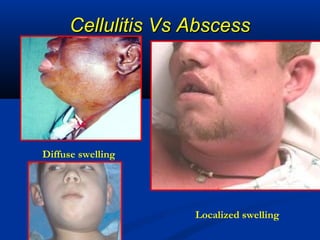
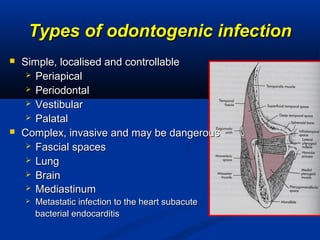
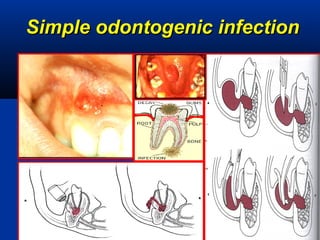
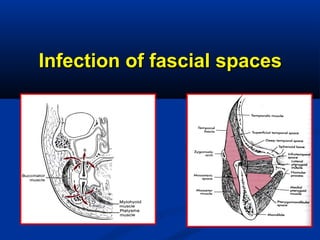

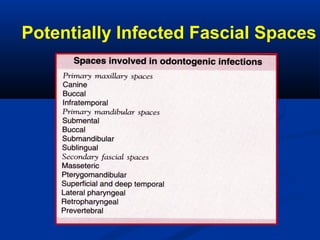



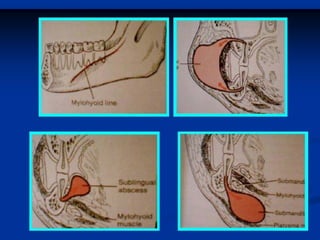
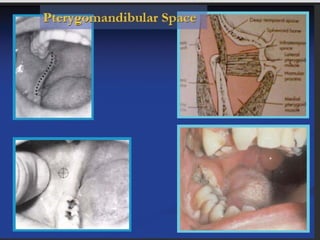
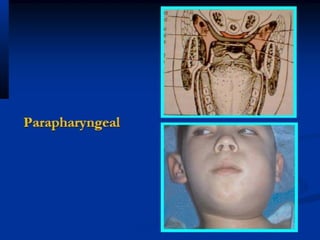

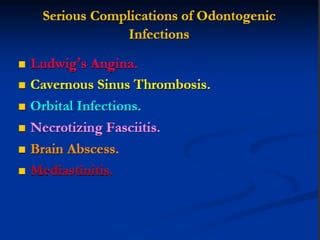

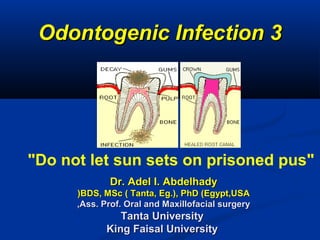









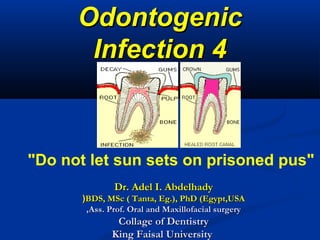

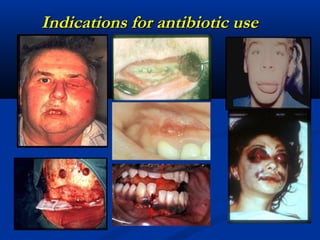



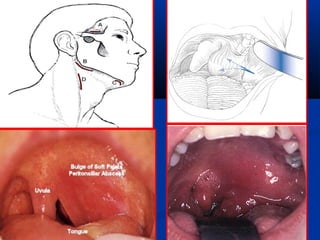
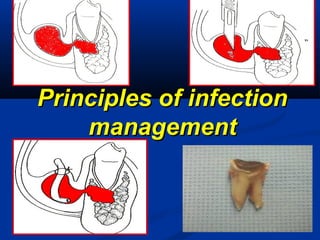

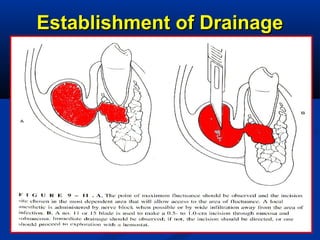
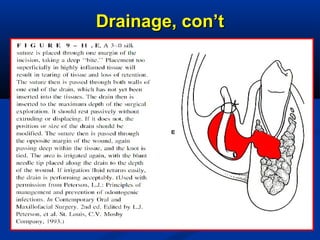




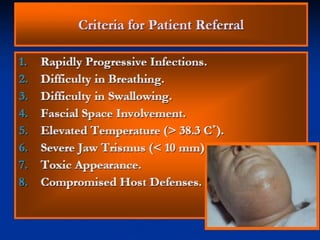

















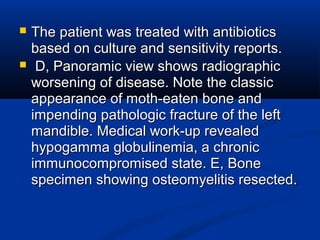
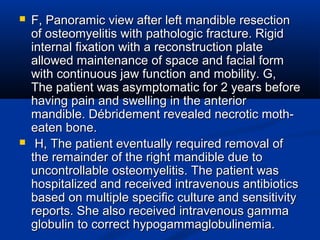
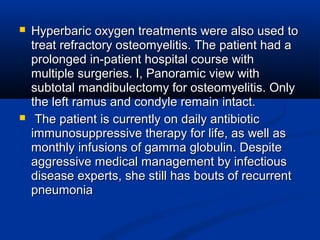




Odontogenic infections are caused by oral bacteria and can spread locally or systemically if not properly treated. Clinical signs may include pain, swelling, erythema, pus formation and fever. Management involves identifying the source, administering antibiotics, and potentially incision and drainage for more severe cases. It is important to promptly treat all odontogenic infections to prevent complications like spread to deep facial spaces.










































































































