Downloaded 1,307 times

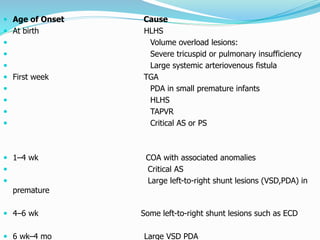

Congestive heart failure occurs when the heart is unable to pump enough blood to meet the body's needs. It can be caused by conditions present at birth like hypoplastic left heart syndrome. Symptoms include poor weight gain, fast breathing, and edema. Diagnosis involves chest x-ray, electrocardiogram, echocardiogram, and sometimes cardiac catheterization. Treatment focuses on underlying causes, medications to control symptoms like diuretics and digoxin, and surgery when possible to correct structural heart defects.