Downloaded 992 times

























![Asbestos-related diseases
Benign
Pleural diseases
1.plaques
2.diffuse pleural thickening
3.effusion
4.calcification
Parenchymal diseases
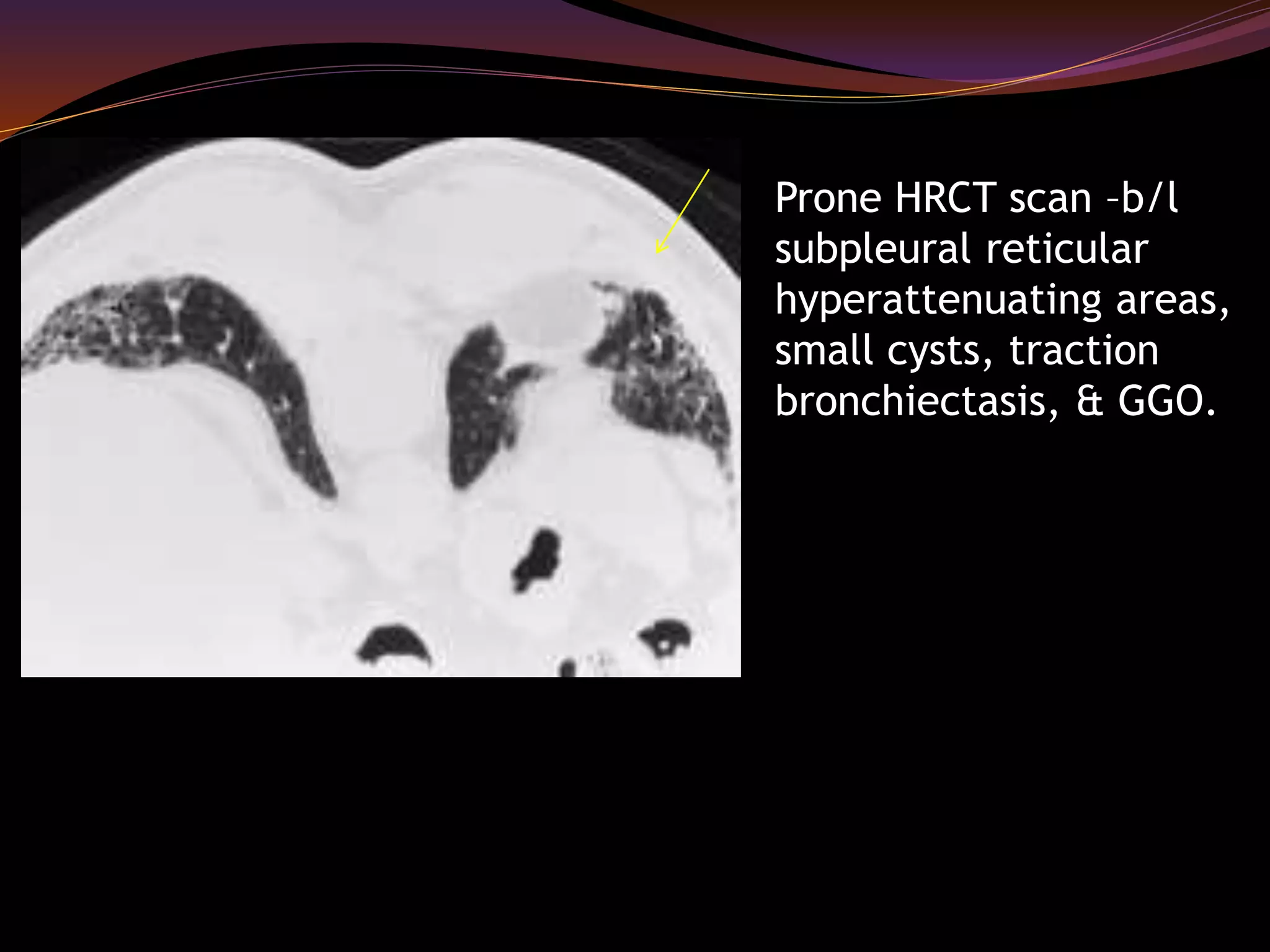
1.Asbestosis [parenchymal
fibrosis caused by asbestos
inhalation]
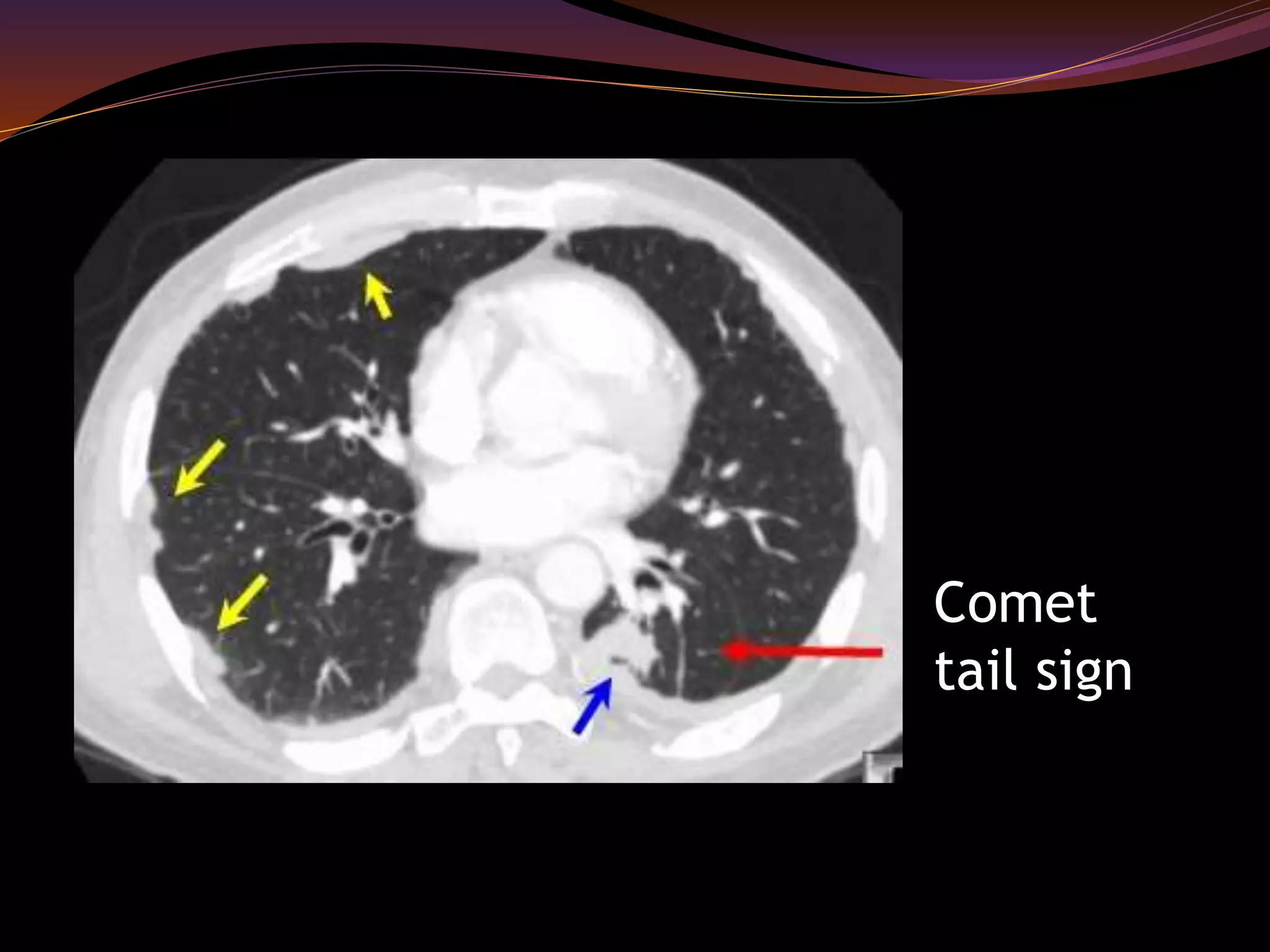
2.Rounded atelectasis
3.Benign fibrotic masses
4.Transpulmonary bands
Malignancy
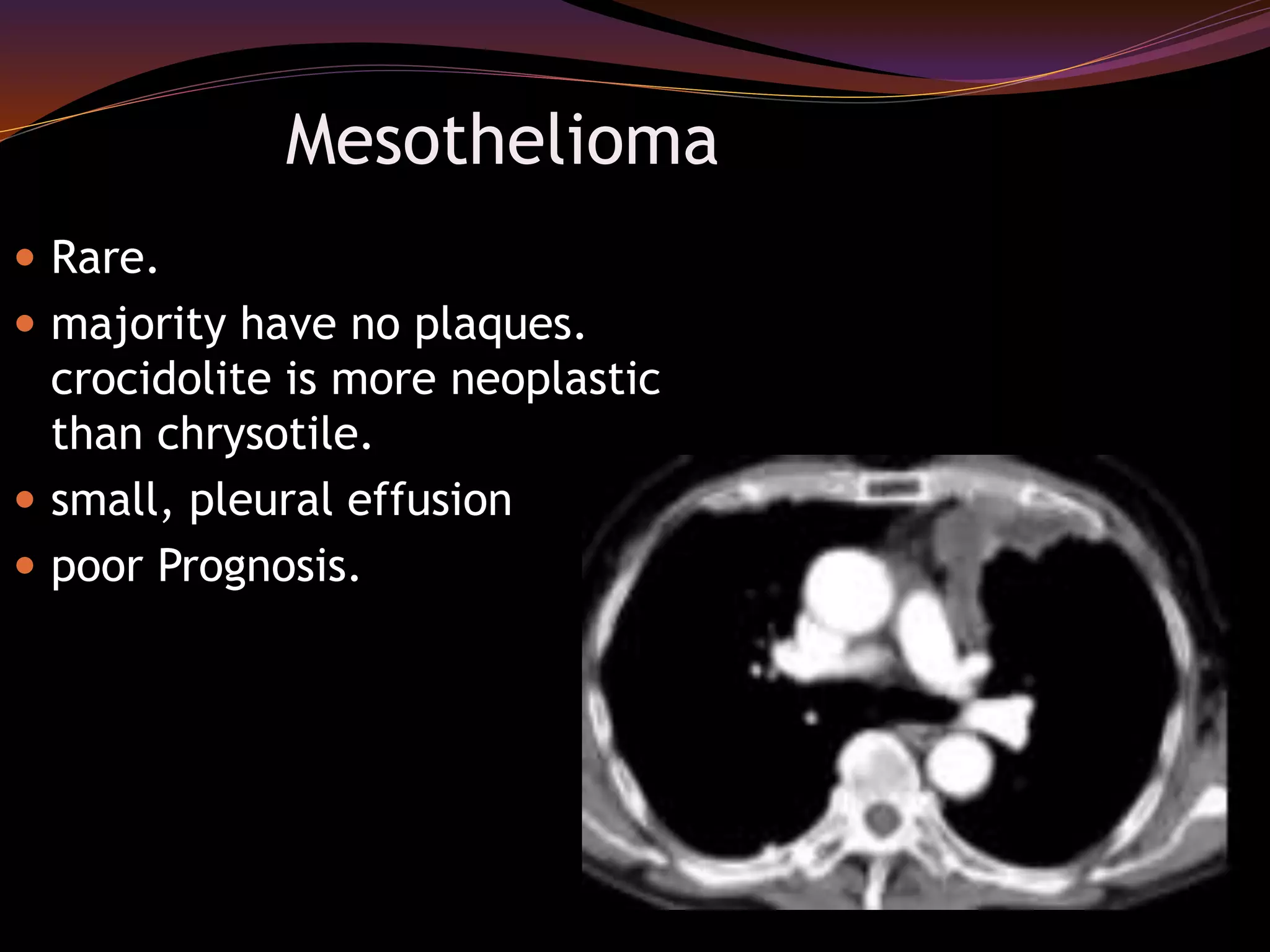
1.Malignant mesothelioma
2.Bronchogenic carcinoma](https://image.slidesharecdn.com/occupationallungdiseases1-141009083912-conversion-gate01/75/Occupational-lung-diseases-radiology-32-2048.jpg)
























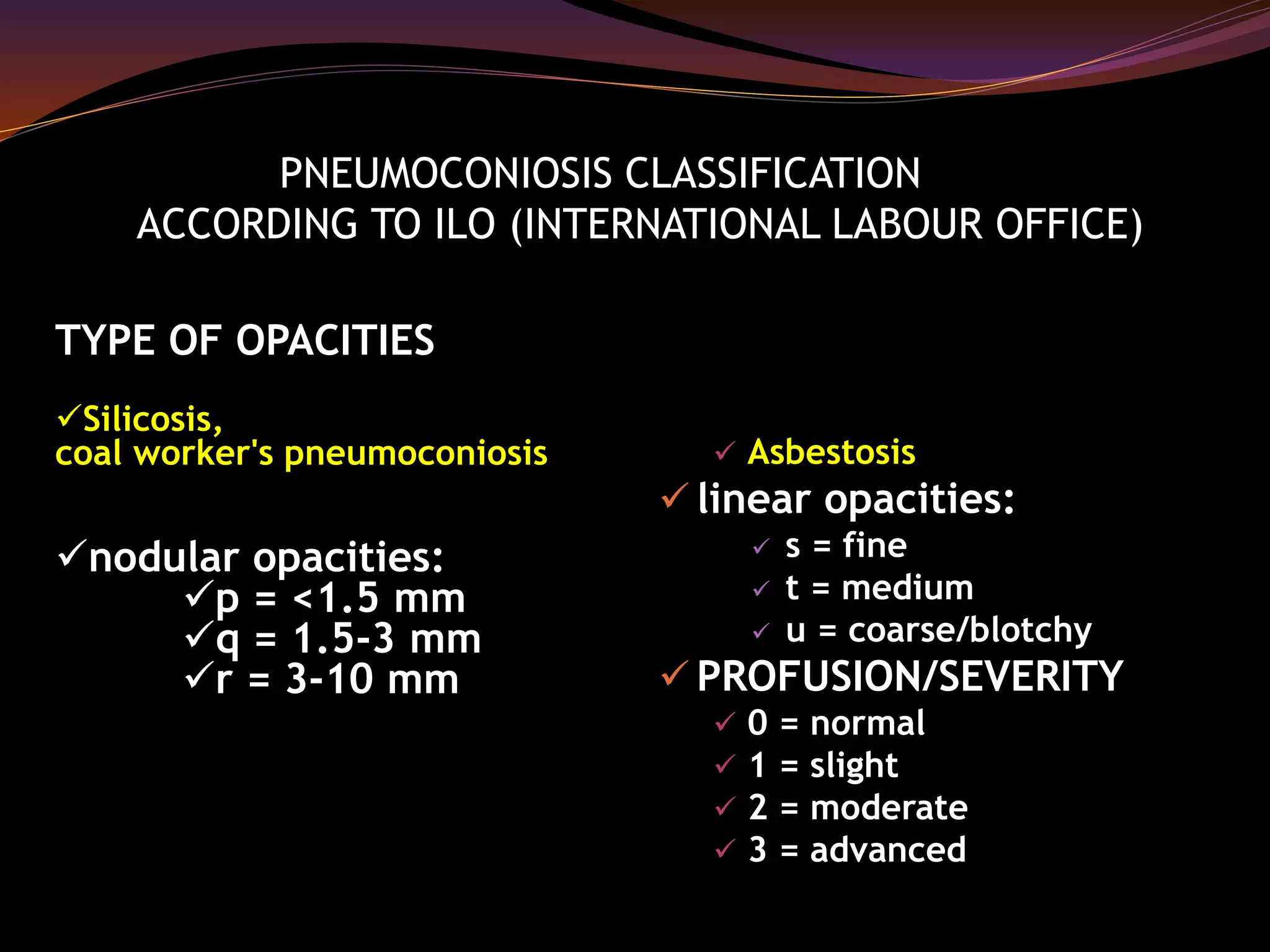
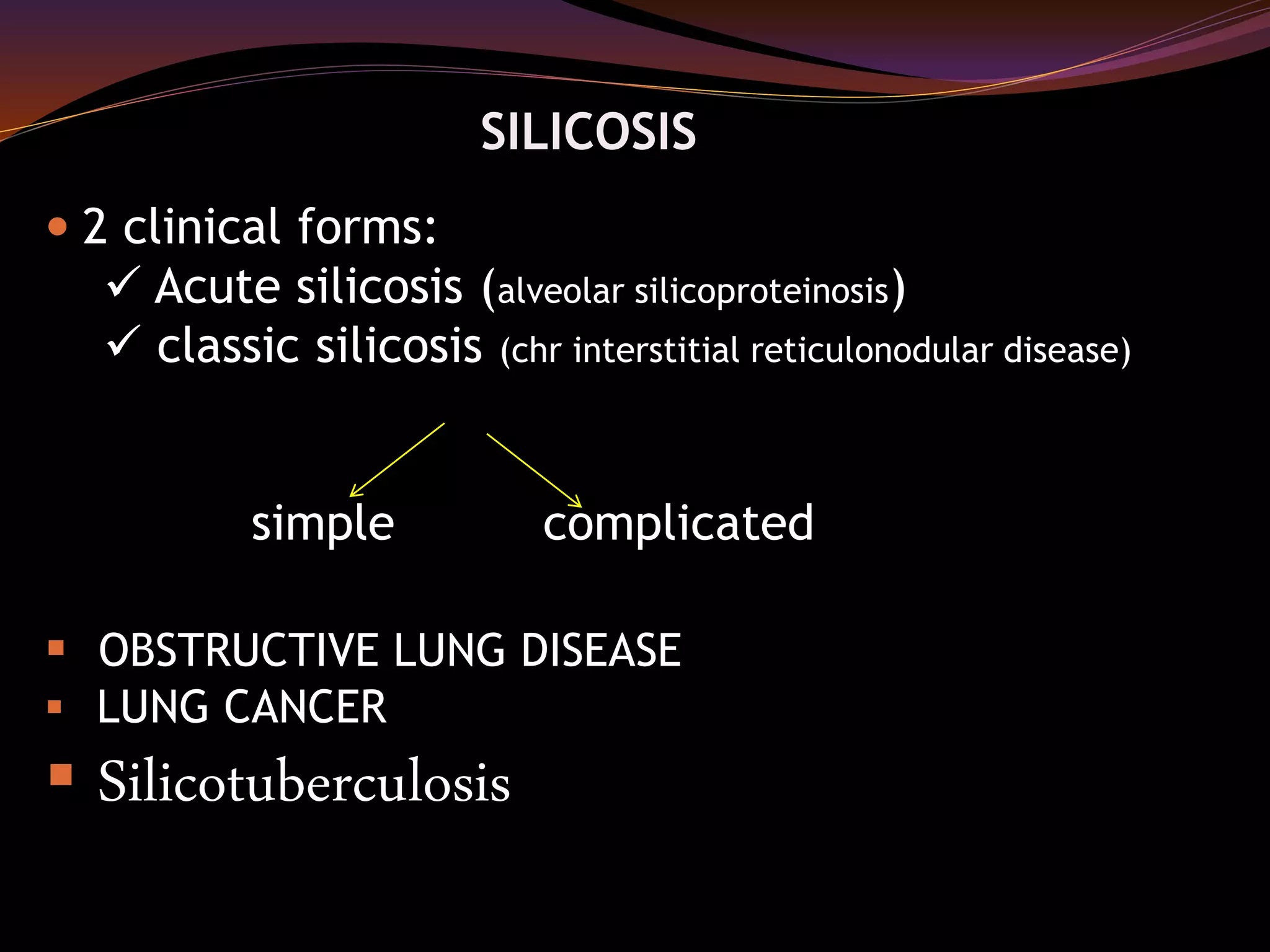
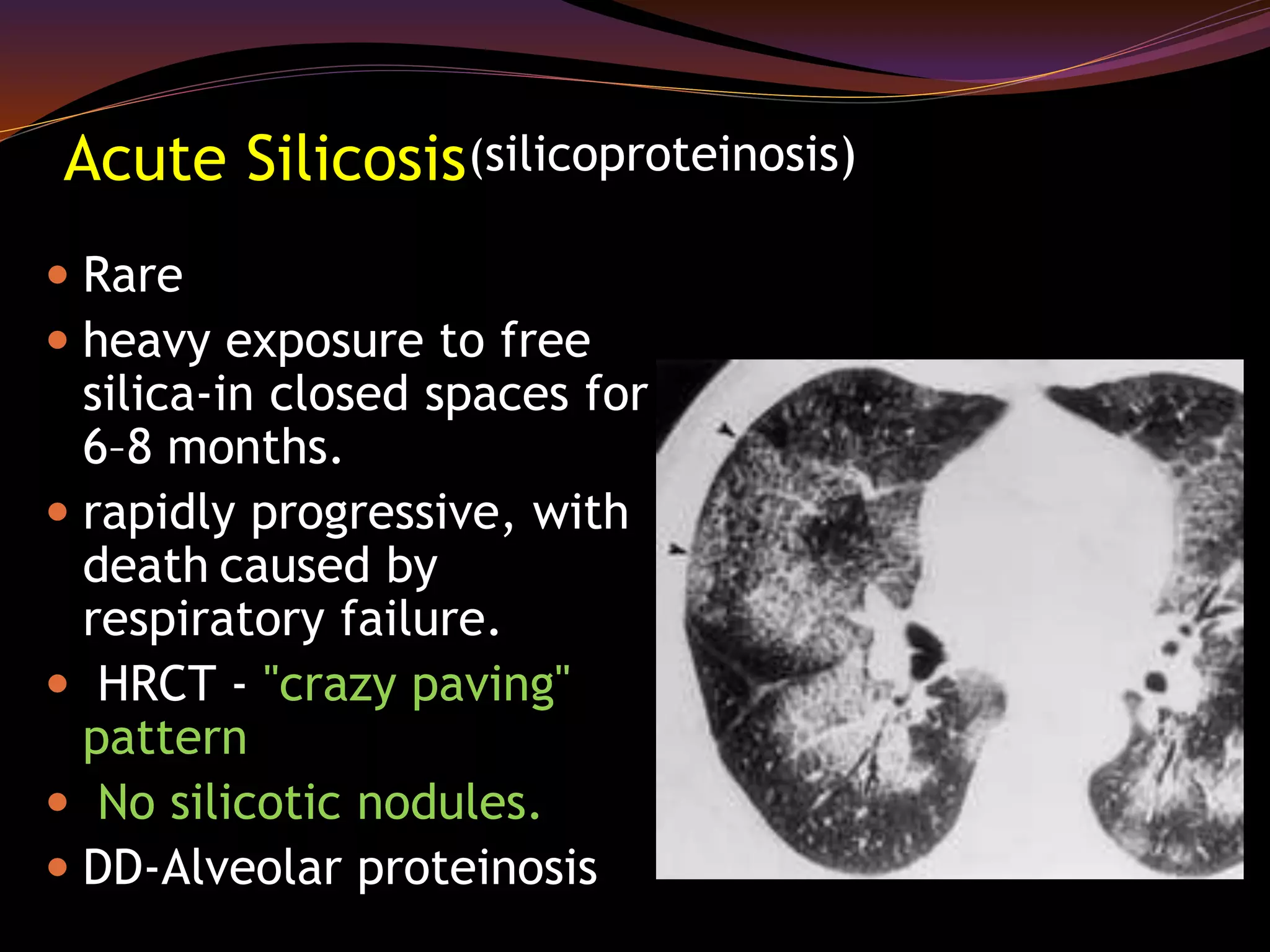
This document discusses occupational lung diseases including pneumoconiosis. It describes the classification of pneumoconiosis according to the ILO including types of opacities seen in conditions like silicosis and asbestosis. It then discusses specific lung diseases caused by occupational exposures like silicosis seen in miners, asbestosis seen in construction workers, and coal worker's pneumoconiosis. Radiologic findings and pathologies of these conditions are summarized along with similarities and differences between diseases like asbestosis and idiopathic pulmonary fibrosis. Occupational lung cancers and mesothelioma caused by asbestos exposure are also mentioned.