Download as PDF, PPTX























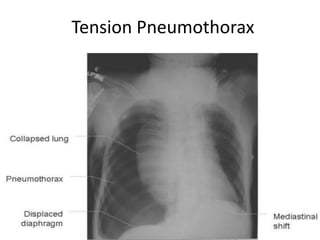




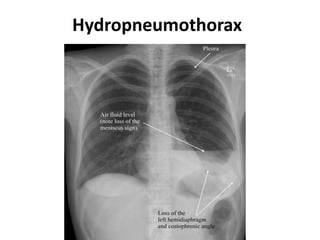



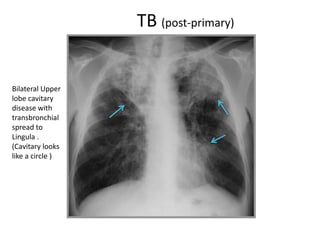


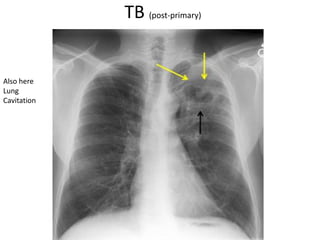





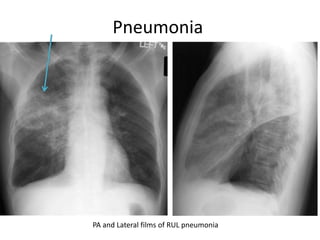

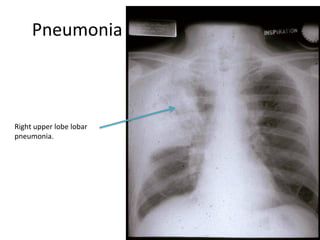








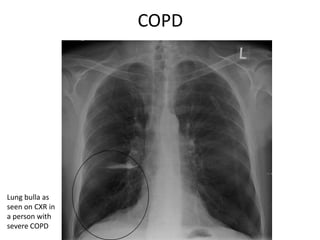



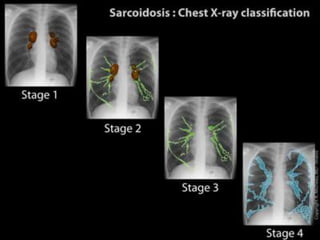


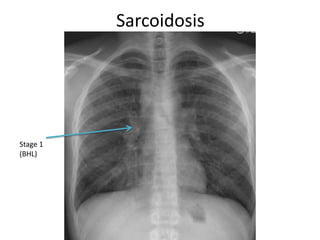


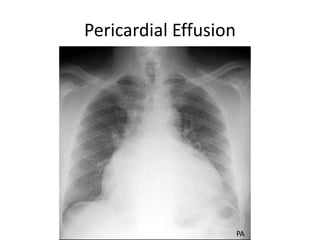


This document provides a summary of key findings that may be seen on chest x-rays. It begins with examples of normal chest x-rays and describes the basic knowledge needed to interpret x-rays. It then discusses specific lung diseases and findings, including pleural diseases, pneumothorax, tuberculosis, pneumonia, interstitial pulmonary fibrosis, COPD, sarcoidosis, and pericardial effusion. Each section provides examples of chest x-rays demonstrating the relevant findings. The document is intended as a study aid for medical exams.






















































![Radiological_diagnosis_of_TB_ECHO_MOH[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/radiologicaldiagnosisoftbechomoh1-240905083452-eb26e5f9-thumbnail.jpg?width=640&height=640&fit=bounds)



















































