Downloaded 49 times

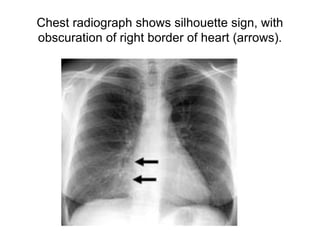
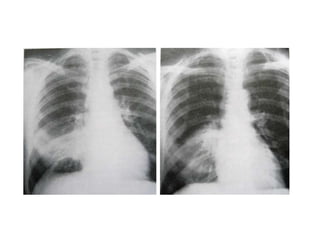

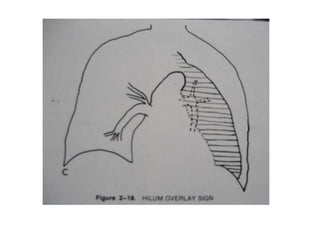
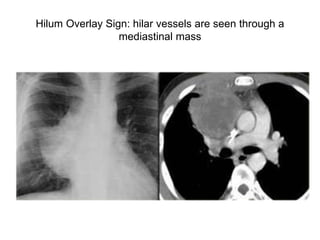



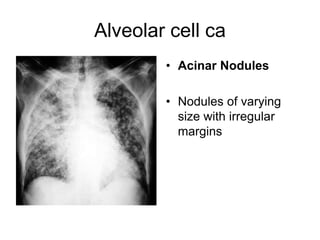
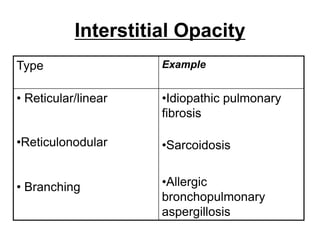
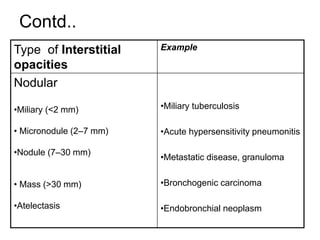
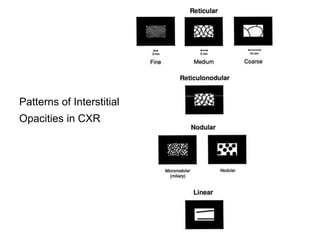
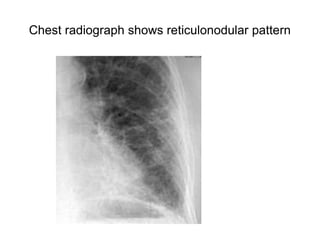
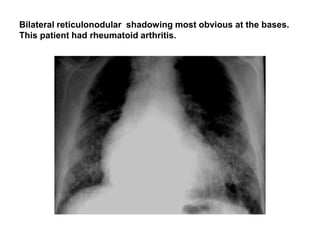
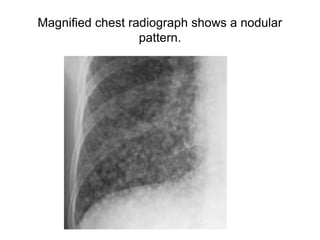
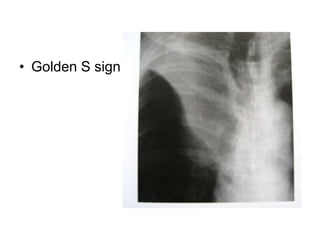
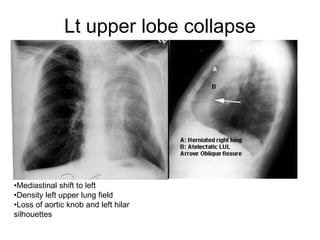

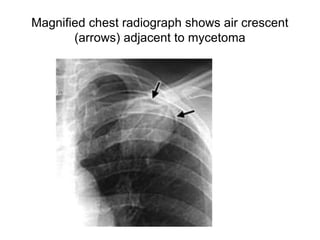
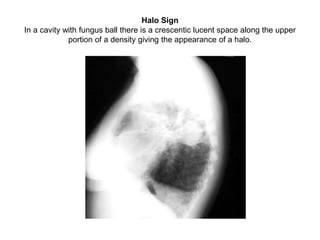

The document discusses various radiographic signs seen on chest x-rays. It describes signs such as the silhouette sign which indicates loss of contrast between adjacent structures, the hilum overlay sign which shows hilar vessels through a mediastinal mass, and air bronchograms which depict air-filled bronchi within consolidated lung. It also covers patterns of parenchymal opacities including alveolar, interstitial and nodular patterns, as well as signs of lung collapse like fissure deformities and compensatory lung changes. Specific findings like the luftsichel sign of left upper lobe collapse and the air crescent sign seen in fungal infections are also summarized.