Downloaded 528 times
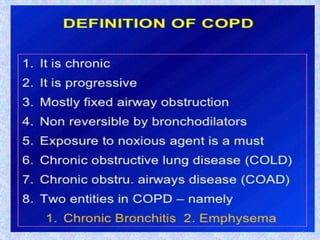
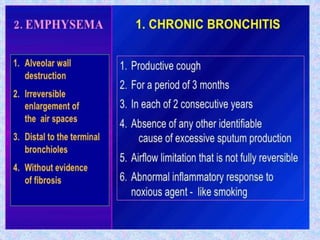
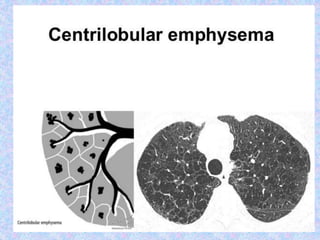
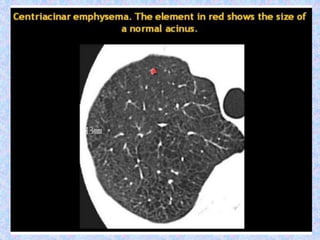
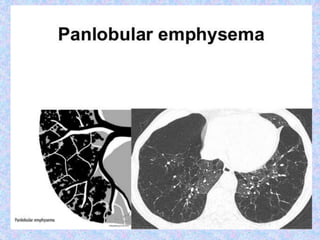
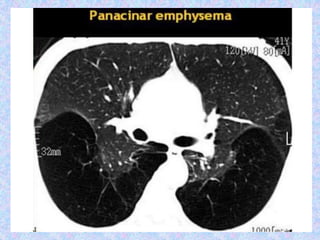
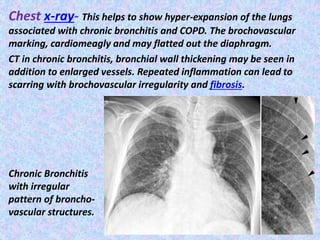
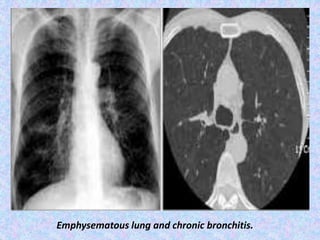
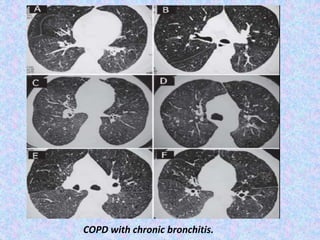
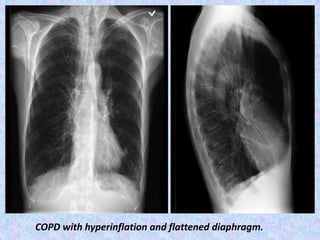
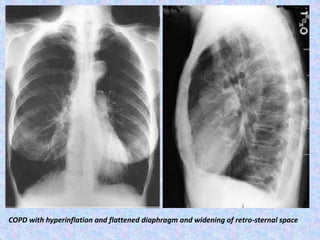
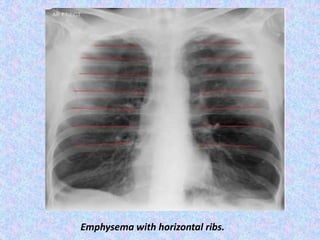
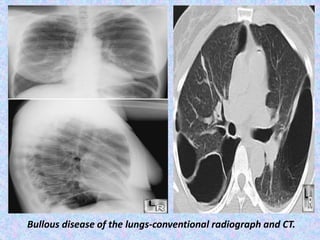
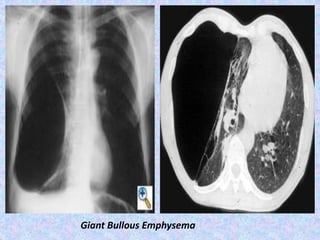
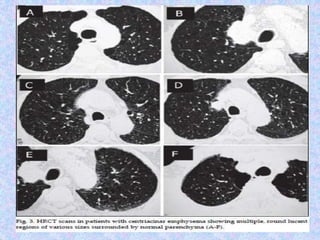
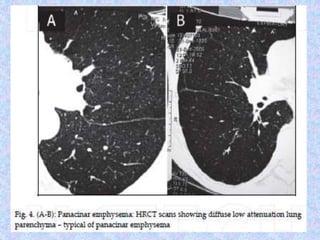
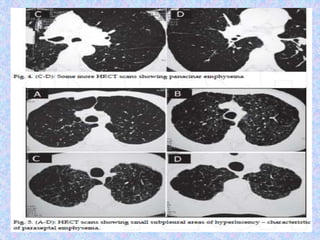
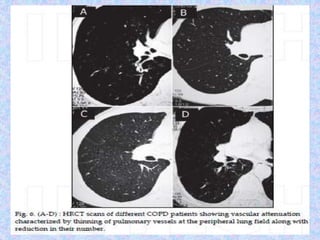
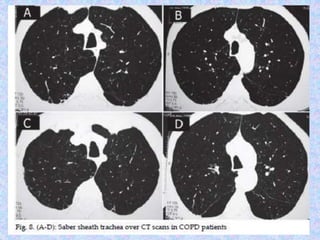
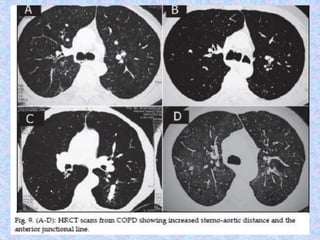
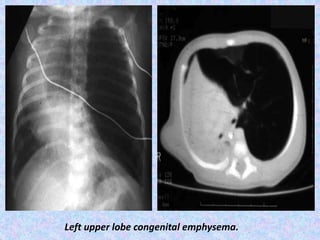
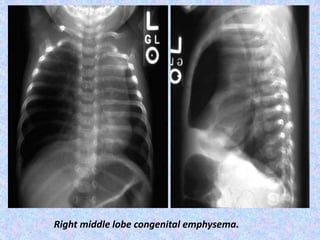
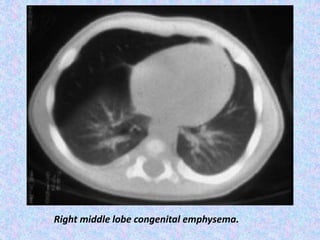
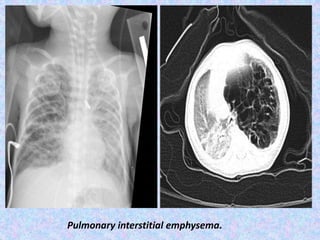
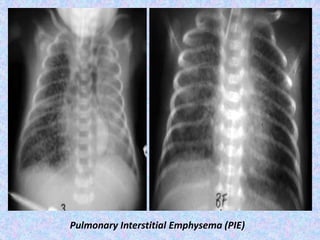
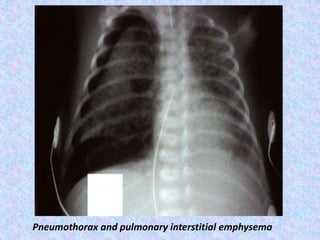
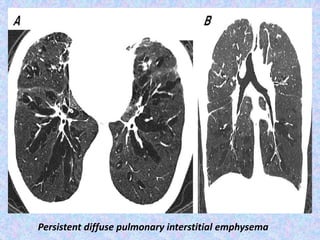
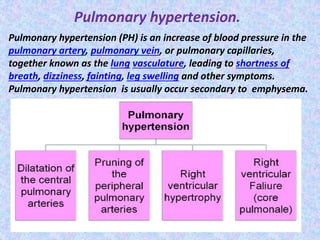
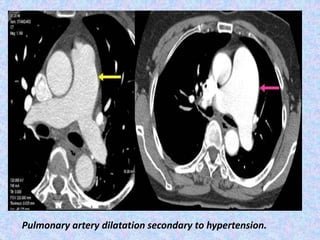
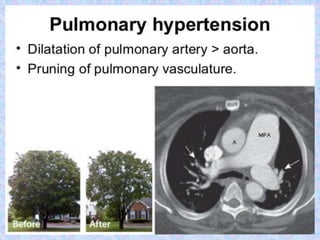
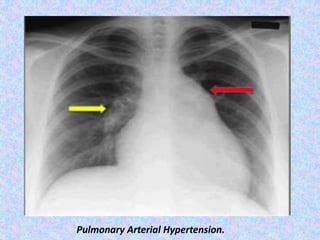

This document discusses radiological imaging findings for various chronic obstructive airway diseases. Chest x-rays and CT scans can show features of chronic bronchitis like bronchovascular thickening and markings. Emphysema appears on imaging as alveolar destruction and airspace enlargement. Bullous lung disease involves air collections like bullae. Congenital lobar emphysema involves overinflation of one or more lobes. Pulmonary interstitial emphysema shows air within the pulmonary interstitium. Pulmonary hypertension can be seen as enlargement of the pulmonary arteries.