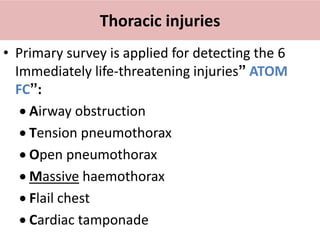
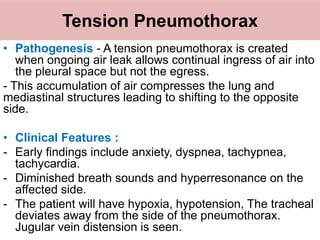
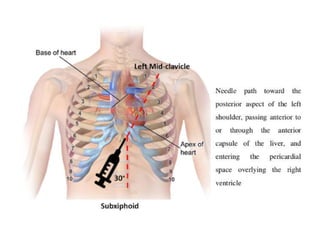
Chest trauma can involve injuries to the chest wall or internal organs. The primary survey focuses on life-threatening injuries like tension pneumothorax, massive hemothorax, or cardiac tamponade. Tension pneumothorax requires immediate needle decompression while massive hemothorax may require a chest tube or thoracotomy. Cardiac tamponade is treated with pericardiocentesis if due to blunt trauma or urgent surgery if from penetrating trauma. The secondary survey entails a full examination to identify injuries like lung contusions or aortic disruption that require further treatment or monitoring.



























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)


![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)












