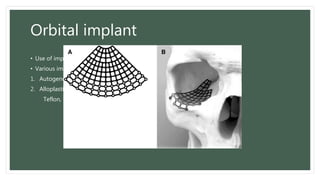
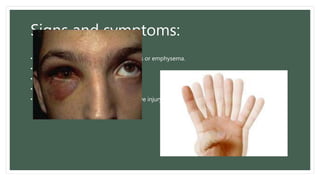
An orbital blowout fracture is caused by blunt force impact to the eye socket, resulting in a fracture of the orbital floor or medial wall. This allows herniation of soft tissues like muscle and fat into the maxillary sinus. Symptoms include double vision, eye movement limitations, and numbness. Diagnosis involves imaging like CT scan to view the "teardrop" sign of herniated tissues. Treatment depends on symptoms but may involve surgery to repair the fracture with implants and release entrapped muscles. Complications can include sunken eyes, double vision, and graft issues if surgery is performed.

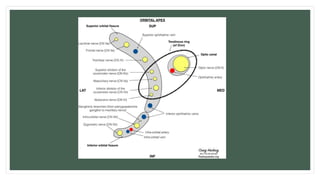

![Clinical significance of intra-orbital
structures:-
• II = Optic (vision)
• III = Oculomotor nerve (Motor)
double vision (diplopia)
eyelid drooping (ptosis)
pupil dilation (mydriasis)
• IV = Trochlear nerve (Motor) Sup. Oblique muscle
Double vision (diplopia) Squint [lateral superior]
• VI = Abducens nerve. Lateral Rectus M
Double vision (diplopia) Squint.[medial]
• V1 = Ophthalmic (Sensory) Corneal anaesthesia.
• V2 = Infra-Orbital (Sensory)
Skin of lower eye lid-nose-upper lip.](https://image.slidesharecdn.com/blowoutfracture-210828000905/85/Blowout-fracture-10-320.jpg)