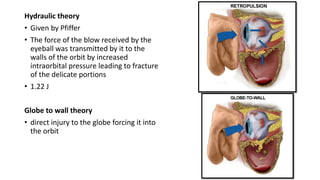
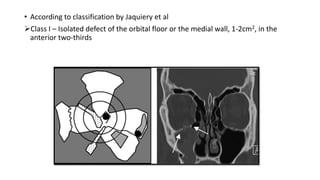
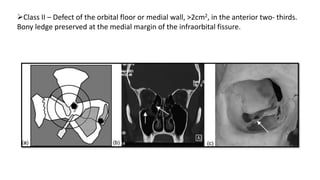
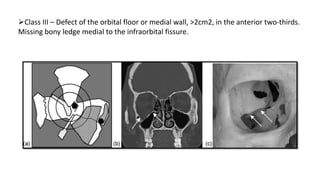
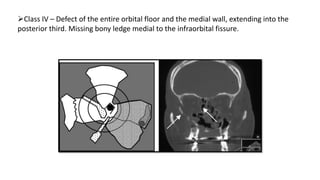
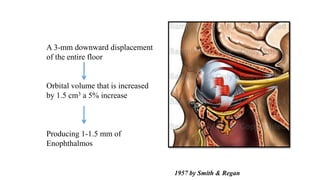
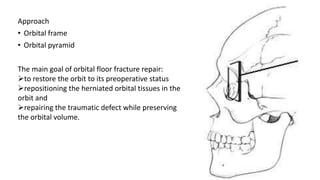
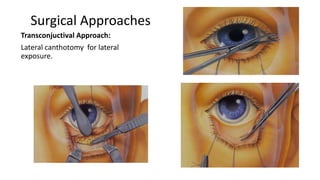
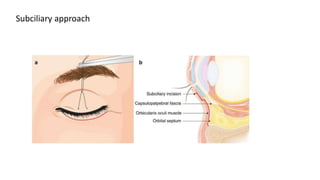
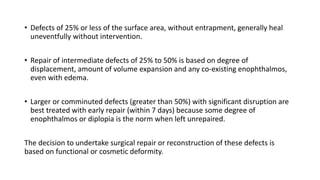
Orbital blowout fractures occur when a sudden increase in intraorbital pressure causes fractures of the orbital floor or medial wall. This allows orbital contents to herniate into the maxillary sinus. Clinical presentation may include diplopia, enophthalmos, numbness, and eye mobility restrictions. Imaging such as CT scans is used to classify the fracture. Early surgical repair within 7-10 days is usually indicated for fractures over 50% of the orbital floor to restore orbital volume and position of tissues. Approaches include transconjunctival or subciliary. The goal of surgery is anatomical reconstruction to restore normal eye position and protect the globe.