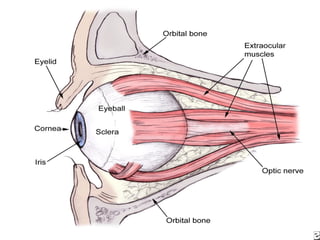
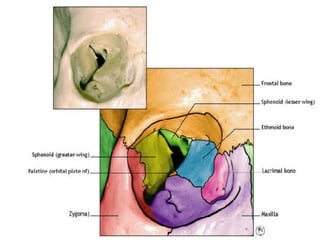
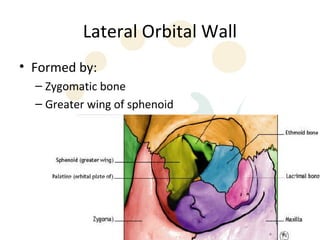
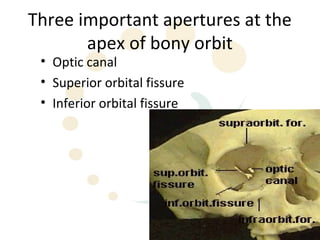
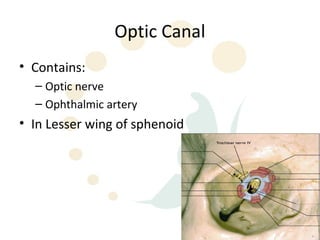
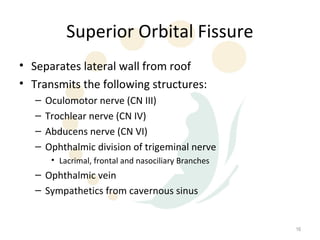
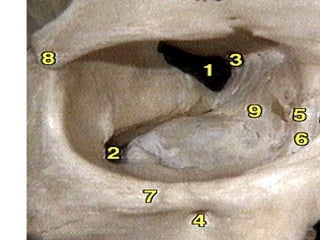
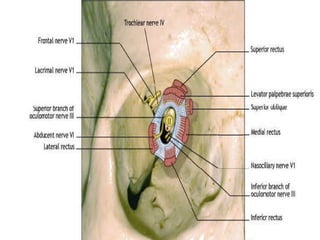
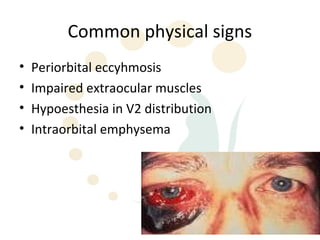
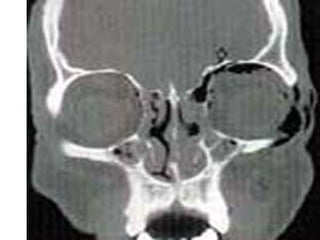
Orbital fractures involve breaks in the bones surrounding the eye socket. The orbital anatomy consists of 7 bones that form the pyramid-shaped orbit. Common types of orbital fractures include fractures of the orbital floor, medial wall, and lateral wall. Signs and symptoms vary depending on the structures involved but may include diplopia, limited eye movement, numbness, and vision changes. Evaluation involves history, exam of cranial nerves and eye movement, and CT scan. Treatment depends on findings but may involve initial management with ice and antibiotics followed by surgery to repair the fracture if indicated to address issues like diplopia or enophthalmos. Surgical approaches and potential complications are discussed.