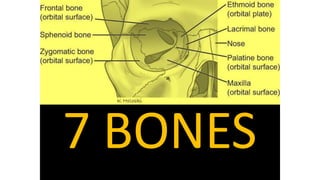
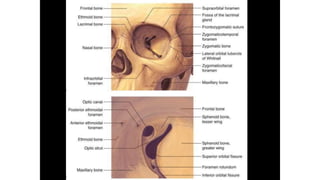
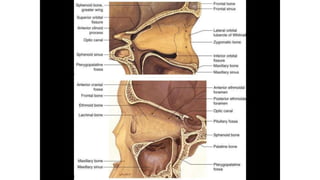
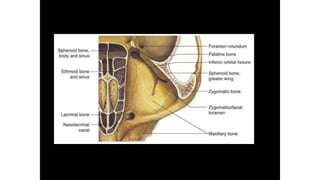
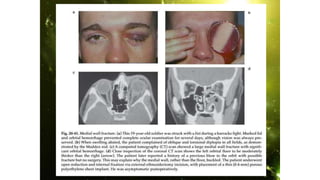
Orbital trauma can cause fractures of the facial bones and soft tissue injuries to the orbit and surrounding structures. Common types of orbital fractures include orbital floor fractures, which result from blows to the orbital rim and are the most frequent. Other types are orbital roof fractures from high impact injuries, medial orbital fractures involving the ethmoid and lacrimal bones, and fractures of the zygomaticomaxillary complex. Clinical examination and imaging studies are used to evaluate the injuries and complications, which may include diplopia, enophthalmos, orbital hemorrhage, and nerve damage. Most isolated floor fractures can be managed conservatively but indications for surgery include restricted eye movements, enophthalmos greater than 2mm, and fractures