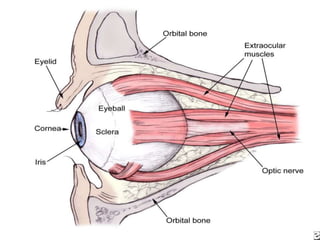
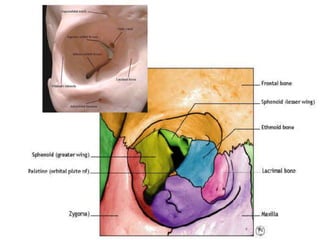
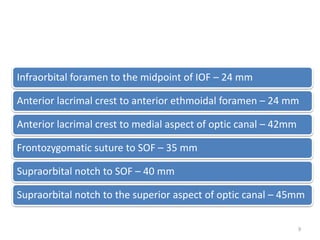
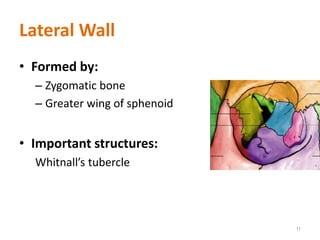
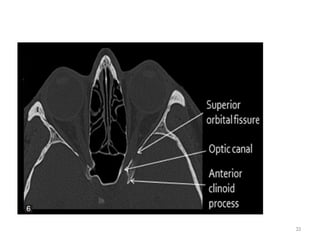
1) The document discusses orbital anatomy and types of orbital fractures. It provides details on the bones that make up the orbital walls and important structures that pass through openings. 2) Common causes of orbital fractures include falling, aggression, sports injuries, and motor vehicle accidents. Signs and symptoms depend on the type and location of the fracture but may include diplopia, limited eye movement, numbness, and vision changes. 3) Treatment involves repairing the fracture through approaches like plate stabilization to restore the orbital walls and prevent complications like enophthalmos.