Downloaded 27 times






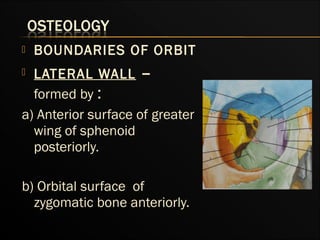





















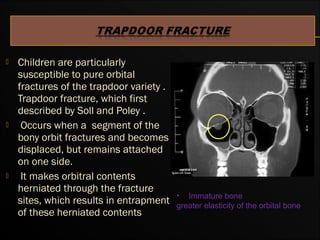



























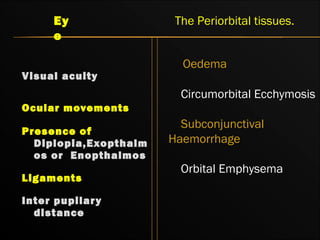







































This document discusses orbital fractures, including: - The surgical anatomy of the orbit and boundaries like the lateral wall and medial wall. - Biomechanics, etiology, fracture patterns, and classification of orbital fractures. - Clinical presentation, diagnosis using imaging like CT, and management including complications. - Recent trends involve use of stereolithography models and computer-assisted reconstruction based on cone beam tomography for complex orbital fractures.












































































