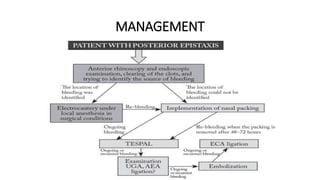
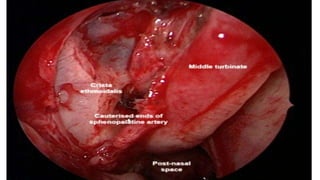
This document discusses Transnasal endoscopic Sphenopalatine artery ligation (TESPAL) as a treatment for refractory epistaxis. It describes the common sites of epistaxis including Little's area and branches of the sphenopalatine artery. TESPAL involves using an endoscope to make an incision near the middle turbinate, retracting tissue to expose the sphenopalatine artery which is then cauterized to stop bleeding. Potential complications include palatal numbness, sinusitis, and septal perforation. TESPAL is indicated for arterial bleeding that is difficult to control with nasal packing.