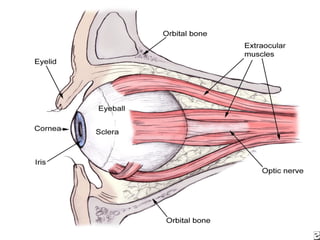
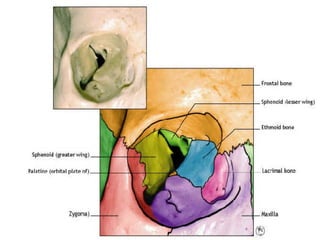
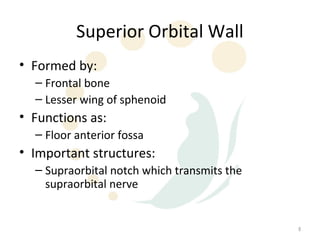
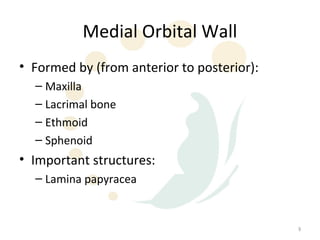
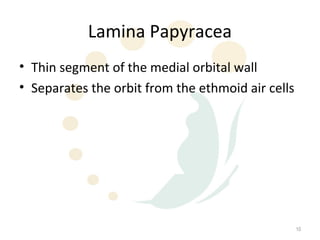
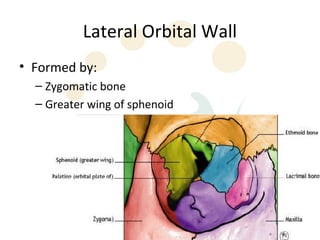
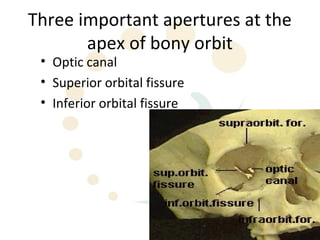
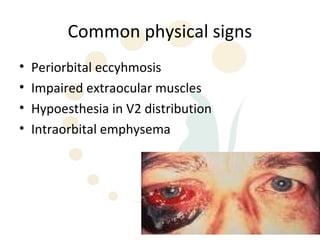
Orbital fractures involve breaks in the bones surrounding the eye socket. The orbit is formed by 7 bones and contains important structures. Types of fractures include those of the orbital floor, walls, and roof. Signs may include bruising, double vision, and numbness. Evaluation involves imaging like CT and examining for vision and eye muscle issues. Treatment depends on severity but may involve monitoring, antibiotics, steroids, or surgery to repair the fracture. Surgical risks include infection, numbness, and rarely blindness.