Downloaded 337 times

























This document discusses diplopia (double vision), including its definition, causes, evaluation, and management. It begins by defining diplopia as seeing double due to misalignment of the eyes. The document then discusses the anatomy involved, types of diplopia (monocular vs binocular), approaches to evaluation, common causes like myasthenia gravis and various cranial nerve palsies, methods of examination, and treatment options which can include patching therapy, addressing underlying causes, eye exercises, and in some cases surgery.
Presentation by Dr. Yugandhar Tummala focusing on diplopia's clinical approach and management.
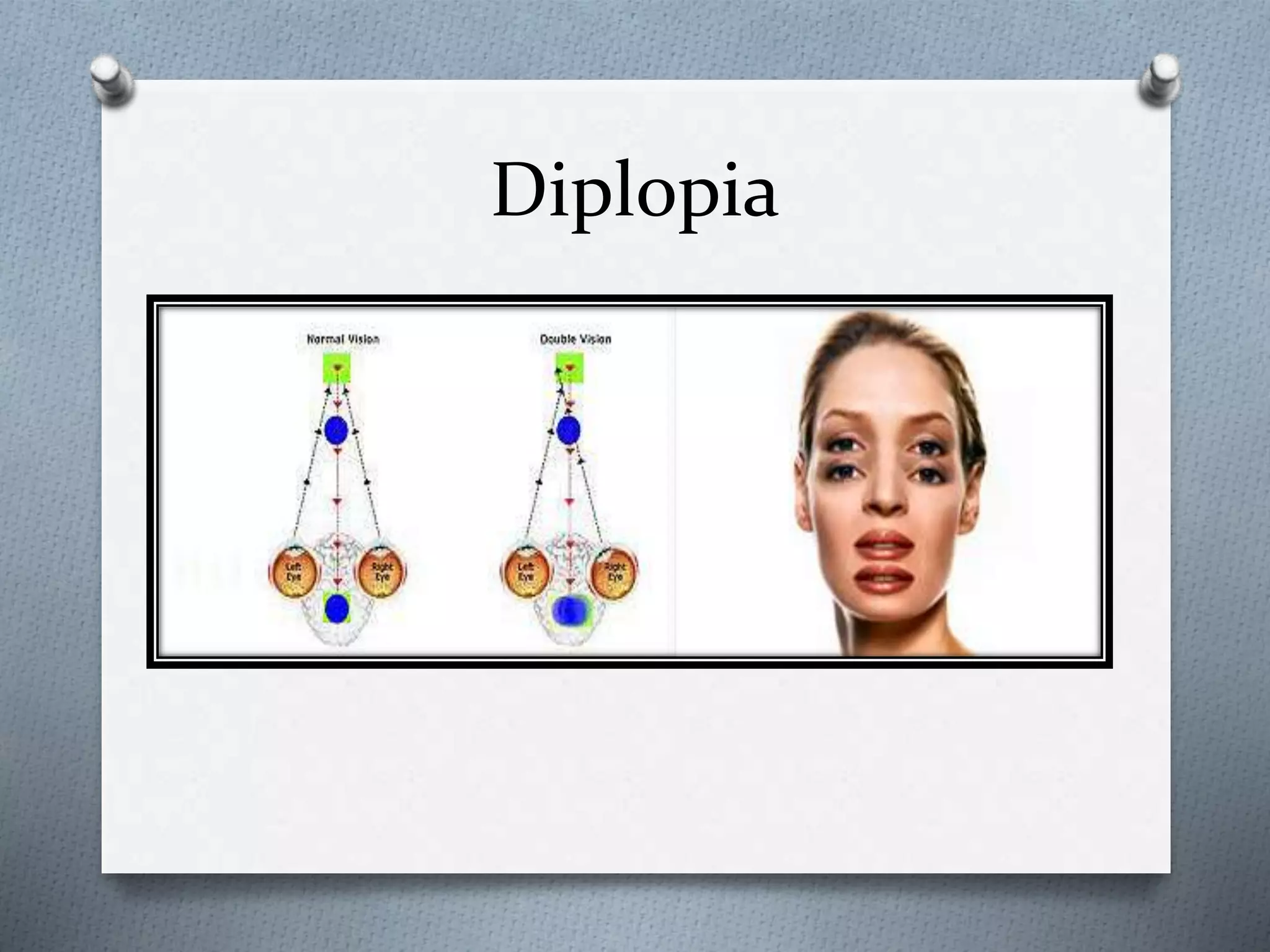
Diplopia refers to double vision caused by misalignment of eyes, leading to two images on the retina.
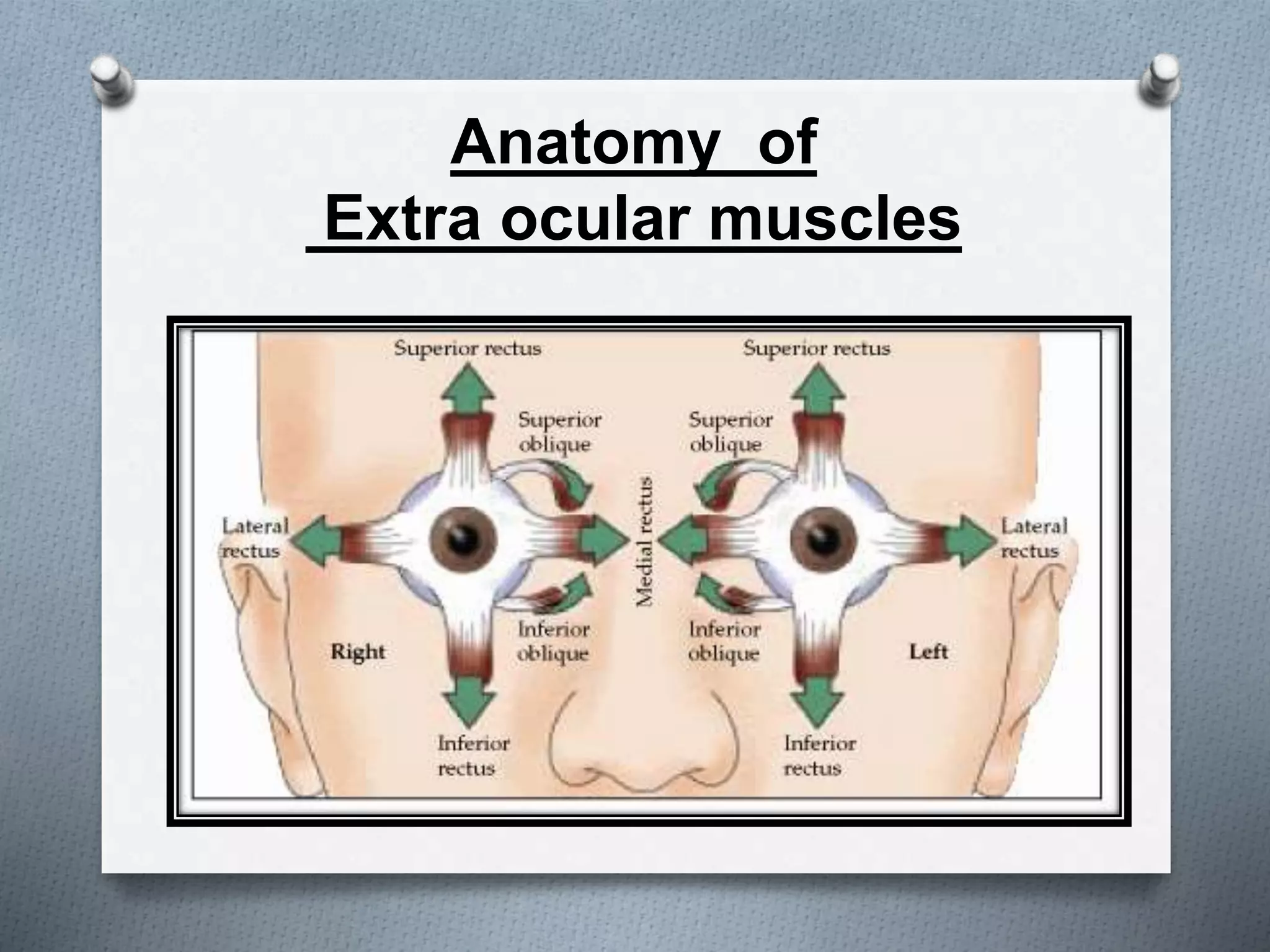
Presentation of the anatomical structure of extraocular muscles involved in eye movement.
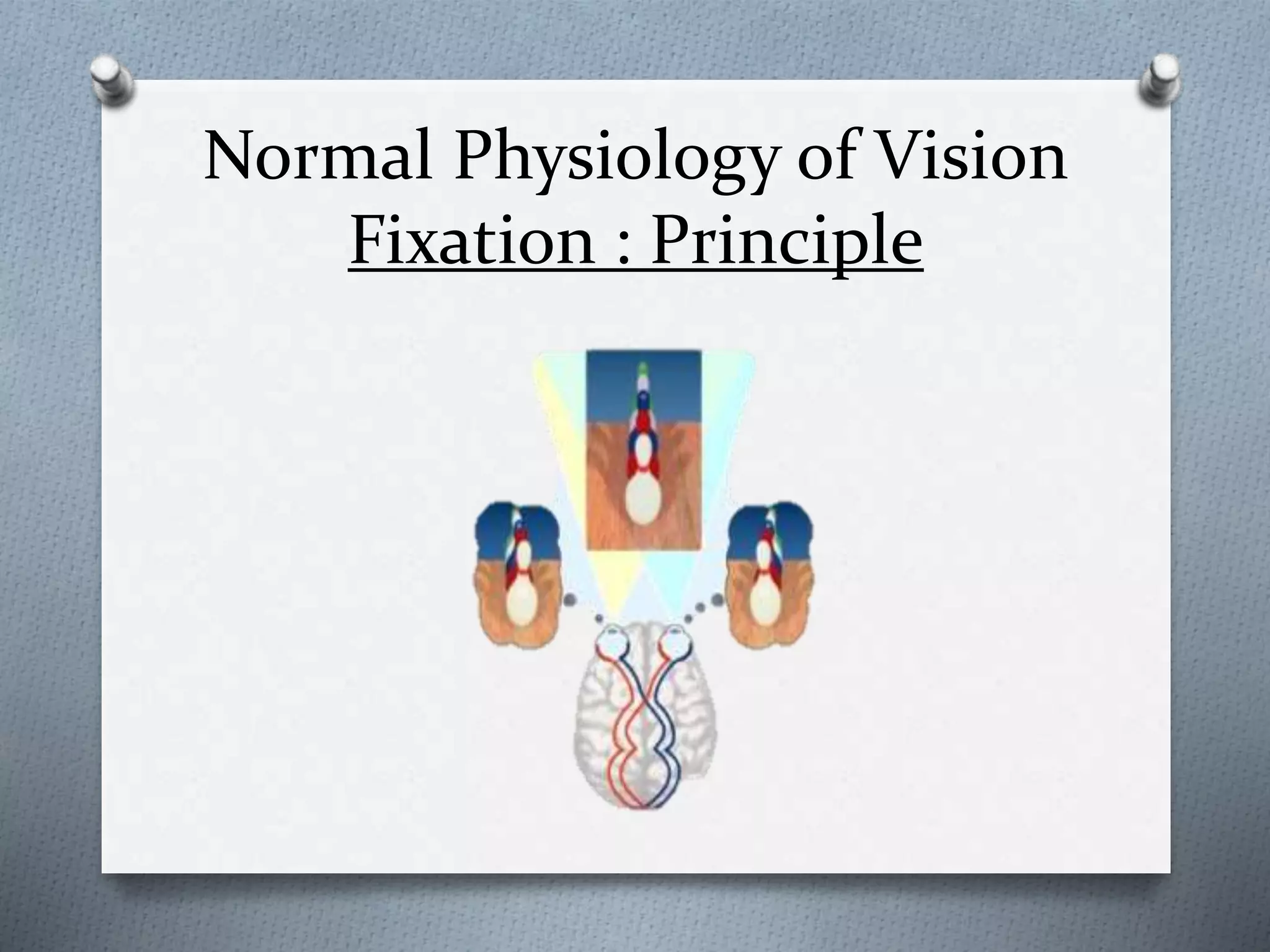
Explanation of the fixation principle and normal vision functioning.
Further discussion on diplopia with potential indications and effects.
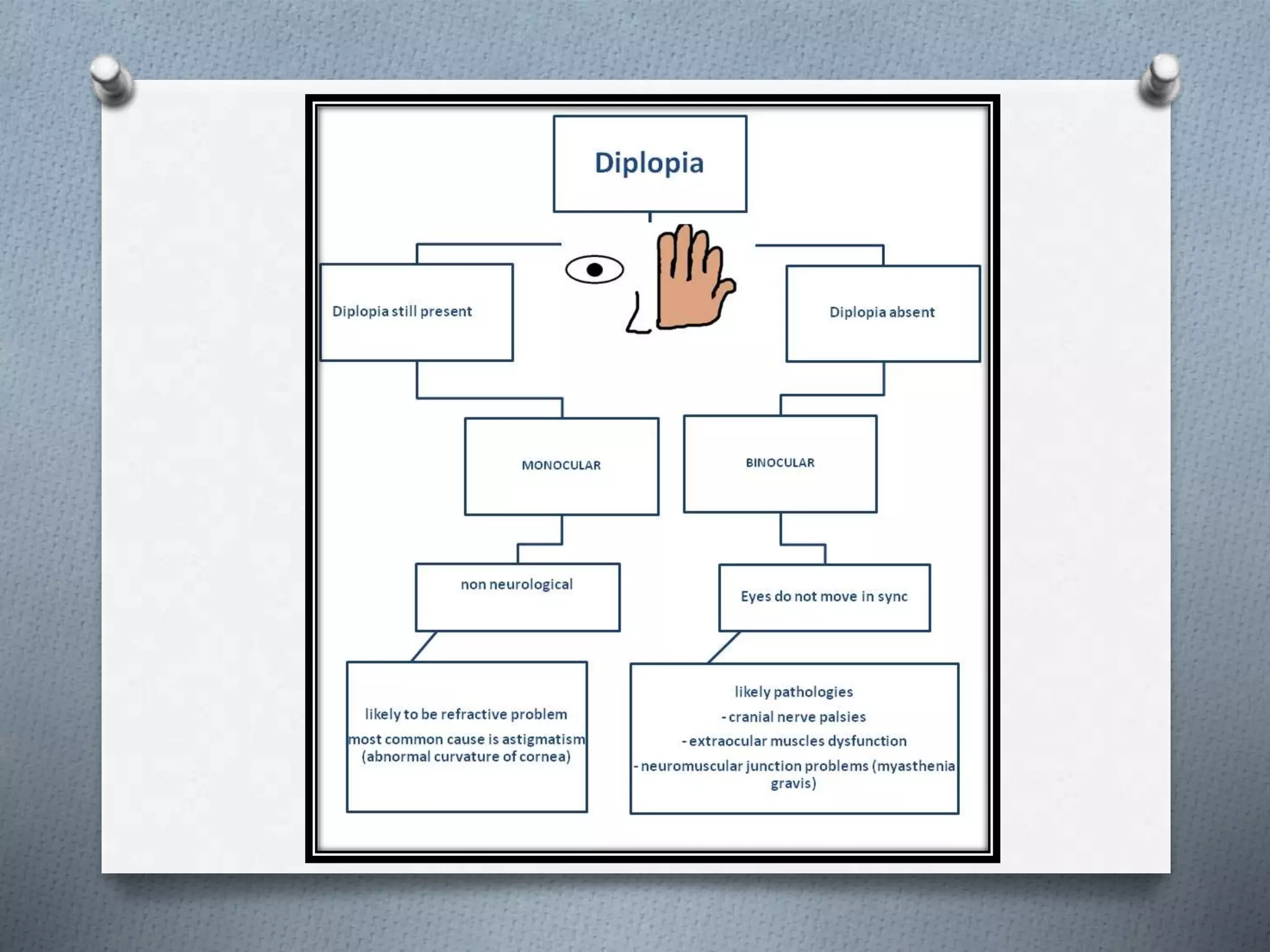
Diplopia evaluation distinguishes between monocular and binocular diplopia, with associated neurological implications.
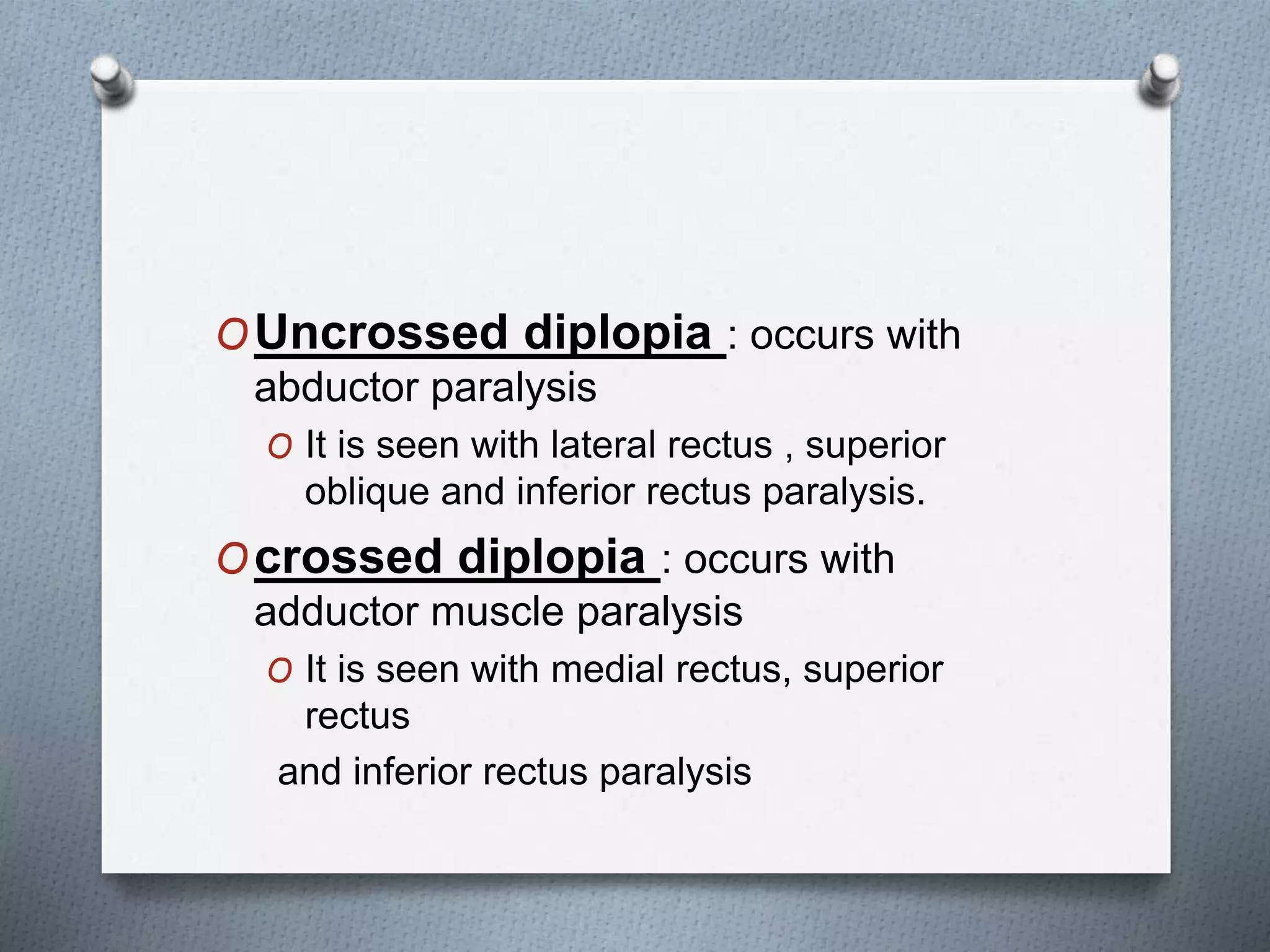
Distinction between uncrossed and crossed diplopia based on muscle paralysis affecting eye movement.
Identifies several causes of monocular diplopia such as dry eyes, corneal opacities, and retinal disorders.
Discusses causes related to the weakness of extraocular muscles and misalignment of images from two eyes.
A clinical case of diplopia linked to Myasthenia gravis indicating symptoms and diagnostic tests.
Myasthenia gravis identified as a significant cause of diplopia with variable symptoms and diagnostic methods.
Rules for analyzing diplopia, addressing image displacement and muscle action in eye movements.
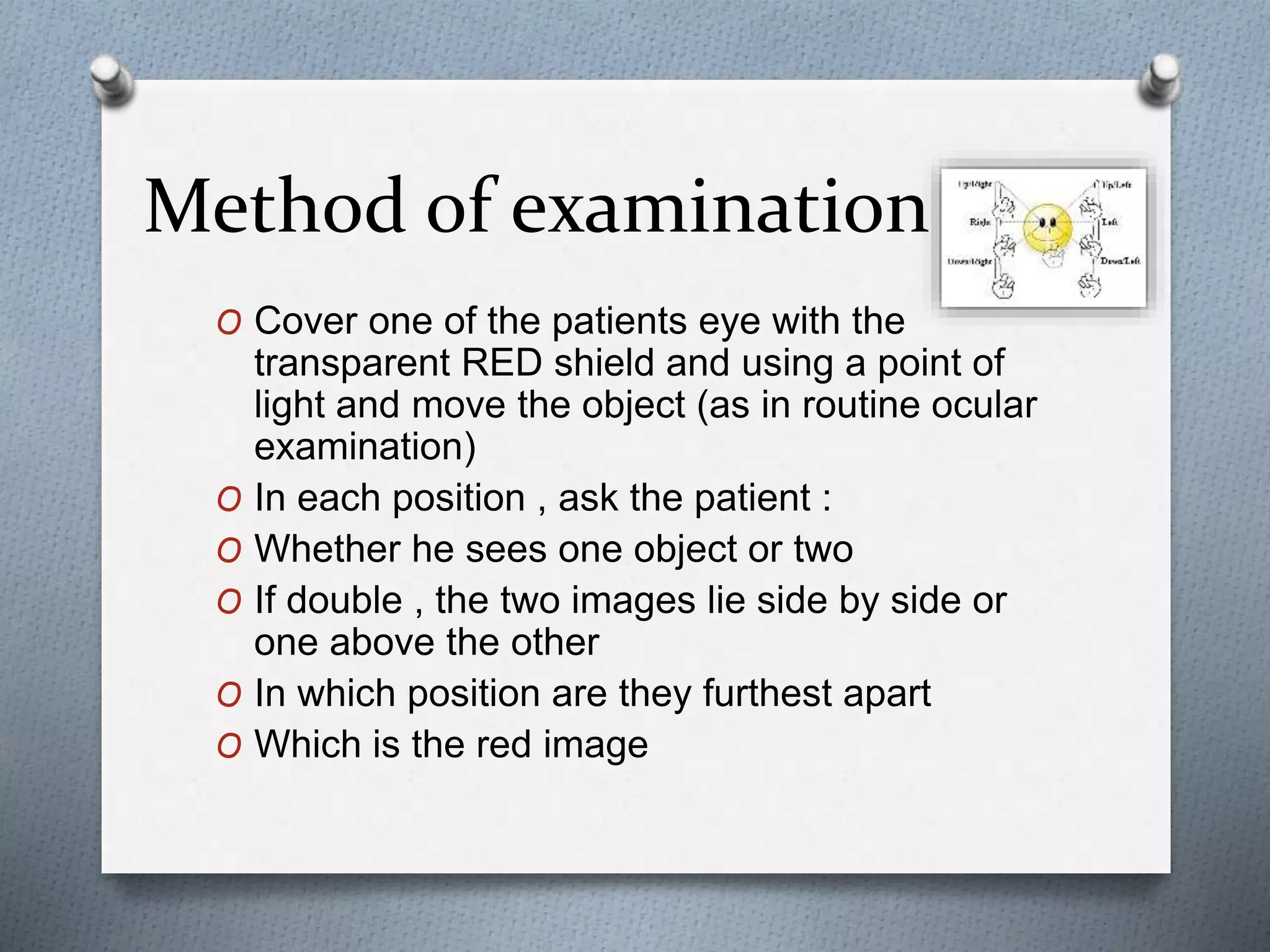
Visual examination techniques using RED shields and light to determine image positioning.
How to interpret the position of overlapping images to ascertain which ocular muscles are defective.
Hirschberg test utilized to evaluate the degree of diplopia via corneal light reflection.
Overview of diplopia charting methods to record observations during examination.
Description of alternating and unilateral cover tests to assess eye alignment and movement.
A subjective test using Maddox rod to detect small ocular deviations and assess alignment.
Comprehensive assessment including patient history, symptom definition, and image separation.
Important observational features in diplopia assessment including head tilt, ptosis, and pupil size.
In-depth eye examination metrics including visual acuity, ocular movement, and alignment.
Approaching diagnosis of diplopia considering onset, variability, pain, and associated symptoms.
Common causes for III, IV, and VI nerve palsies, highlighting significant clinical conditions.
Detailed assessment of third nerve palsy with implications on eyelid paralysis and pupil involvement.
Characterization of trochlear nerve palsy and its diagnostic features related to head positioning.
Details regarding abducens nerve palsy causes, symptoms, and relation to raised intracranial pressure.
Highlighting differentiating features of double vision in varying clinical contexts.
Explanation of intranuclear ophthalmoplegia, its causes, and effects on ocular movement.
Overview of treatment strategies for diplopia including patching, exercises, and surgical options.
List of references used for the presentation on diplopia and its management.























































































