Downloaded 70 times
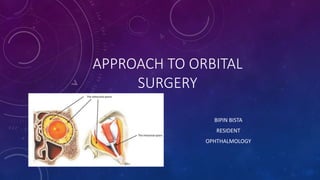

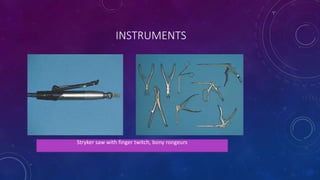






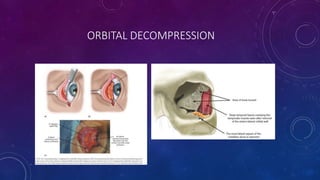
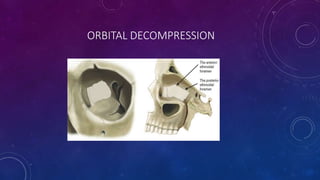




This document provides an overview of approaches to orbital surgery. It discusses the different surgical spaces in the orbit and various instrumentation used. It describes techniques for superior, inferior, medial, lateral, and transcranial approaches. Key steps are outlined for each approach. The document also discusses orbital decompression procedure and postoperative care. Potential complications of orbital surgery are noted. References for further reading are provided.























































































